催乳素 (PRL) 水平升高见于几种生理和病理状态。一项纳入1234 名高泌乳素血症患者的回顾性、多中心研究显示,56.2% 的患者有催乳素瘤,14.5% 的患者有药物引发的高泌乳素血症,9.3% 的患者有巨泌乳素血症,6.6% 的患者有无功能性垂体腺瘤,6.3%的患者有原发性甲状腺功能减退症,3.6%的患者有特发性高泌乳素血症,3.2%的患者有肢端肥大症。[11]Vilar L, Freitas MC, Naves LA, et al. Diagnosis and management of hyperprolactinemia: results of a Brazilian multicenter study with 1234 patients. J Endocrinol Invest. 2008 May;31(5):436-44.http://www.ncbi.nlm.nih.gov/pubmed/18560262?tool=bestpractice.com 因此,高泌乳素血症的病因可以被归类为病理性,生理性,药物性或特发性。
病理性
病理性高泌乳素血症的原因主要是泌乳素分泌性垂体腺瘤(泌乳素瘤)、压迫垂体柄的肿块(由于多巴胺从下丘脑传导到泌乳素细胞受到抑制)、共分泌生长激素 (GH) 的垂体腺瘤、甲状腺功能减退症(由于下丘脑合成促甲状腺激素释放激素升高)以及慢性肾功能衰竭(因为 PRL 清除率降低)。
肿瘤病理学
90% 的催乳素瘤都是催乳素微腺瘤(肿瘤直径<10 mm),占功能性垂体瘤的 25%-30%,是高泌乳素血症最常见的原因。大催乳素瘤(肿瘤直径>10 mm)相对少见,构成催乳素瘤的其余部分。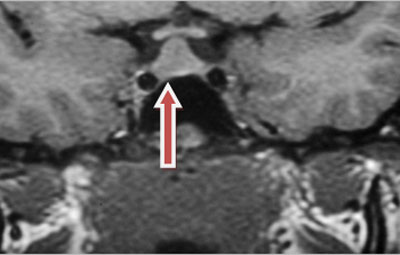 [Figure caption and citation for the preceding image starts]: MRI显示为大泌乳素瘤由 Faidon Harsoulis, MD 提供;经许可后使用 [Citation ends]. 可能是诊断相对比较延迟的原因,大泌乳素瘤更常见于男性。[3]Mah PM, Webster J. Hyperprolactinemia: etiology, diagnosis, and management. Semin Reprod Med. 2002 Nov;20(4):365-74.http://www.ncbi.nlm.nih.gov/pubmed/12536359?tool=bestpractice.com[12]Schlechte JA. Long-term management of prolactinomas. J Clin Endocrinol Metab. 2007 Aug;92(8):2861-5.https://academic.oup.com/jcem/article/92/8/2861/2597201http://www.ncbi.nlm.nih.gov/pubmed/17682084?tool=bestpractice.com 血清PRL水平通常与肿瘤体积匹配,很少见催乳素瘤显著增大,但PRL没有明显增加的情况。
[Figure caption and citation for the preceding image starts]: MRI显示为大泌乳素瘤由 Faidon Harsoulis, MD 提供;经许可后使用 [Citation ends]. 可能是诊断相对比较延迟的原因,大泌乳素瘤更常见于男性。[3]Mah PM, Webster J. Hyperprolactinemia: etiology, diagnosis, and management. Semin Reprod Med. 2002 Nov;20(4):365-74.http://www.ncbi.nlm.nih.gov/pubmed/12536359?tool=bestpractice.com[12]Schlechte JA. Long-term management of prolactinomas. J Clin Endocrinol Metab. 2007 Aug;92(8):2861-5.https://academic.oup.com/jcem/article/92/8/2861/2597201http://www.ncbi.nlm.nih.gov/pubmed/17682084?tool=bestpractice.com 血清PRL水平通常与肿瘤体积匹配,很少见催乳素瘤显著增大,但PRL没有明显增加的情况。
大部分 PRL 水平>6522 pmol/L (150 μg /L) 的患者有催乳素瘤。 巨催乳素瘤患者通常会出现 PRL 浓度>10,870 pmol (250 μg/L),有时>43,478 pmol/L (1000 μg/L)。[1]Casanueva FF, Molitch ME, Schlechte JA, et al. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf). 2006 Aug;65(2):265-73.https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2265.2006.02562.xhttp://www.ncbi.nlm.nih.gov/pubmed/16886971?tool=bestpractice.com[12]Schlechte JA. Long-term management of prolactinomas. J Clin Endocrinol Metab. 2007 Aug;92(8):2861-5.https://academic.oup.com/jcem/article/92/8/2861/2597201http://www.ncbi.nlm.nih.gov/pubmed/17682084?tool=bestpractice.com 存在垂体大腺瘤和轻度高催乳素血症 (<4348 pmol/L [<100 μg/L]) 的患者最有可能存在非分泌性垂体肿瘤,而不是催乳素瘤。[13]Bevan JS, Burke CW, Esiri MM, et al. Misinterpretation of prolactin levels leading to management errors in patients with sellar enlargement. Am J Med. 1987 Jan;82(1):29-32.http://www.ncbi.nlm.nih.gov/pubmed/3799691?tool=bestpractice.com 然而,这些关联并不是绝对的。[1]Casanueva FF, Molitch ME, Schlechte JA, et al. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf). 2006 Aug;65(2):265-73.https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2265.2006.02562.xhttp://www.ncbi.nlm.nih.gov/pubmed/16886971?tool=bestpractice.com[12]Schlechte JA. Long-term management of prolactinomas. J Clin Endocrinol Metab. 2007 Aug;92(8):2861-5.https://academic.oup.com/jcem/article/92/8/2861/2597201http://www.ncbi.nlm.nih.gov/pubmed/17682084?tool=bestpractice.com
大部分催乳素瘤仅分泌 PRL,但是约 10% 的催乳素瘤含有生长激素细胞,因此也会分泌 GH。它们很少产生促甲状腺激素和促肾上腺皮质激素。
累及下丘脑和压迫垂体柄的肿块通常导致 PRL 水平<10,870 pmol/L (250 μg/L)。 这包括非功能性的腺瘤、颅咽管瘤、神经胶质瘤和转移性肿瘤。[1]Casanueva FF, Molitch ME, Schlechte JA, et al. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf). 2006 Aug;65(2):265-73.https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2265.2006.02562.xhttp://www.ncbi.nlm.nih.gov/pubmed/16886971?tool=bestpractice.com[2]Serri O, Chik CL, Ur E, et al. Diagnosis and management of hyperprolactinemia. CMAJ. 2003 Sep 16;169(6):575-81.http://www.cmaj.ca/content/169/6/575.longhttp://www.ncbi.nlm.nih.gov/pubmed/12975226?tool=bestpractice.com[3]Mah PM, Webster J. Hyperprolactinemia: etiology, diagnosis, and management. Semin Reprod Med. 2002 Nov;20(4):365-74.http://www.ncbi.nlm.nih.gov/pubmed/12536359?tool=bestpractice.com
产生 GH 的肿瘤中约 25% 也分泌 PRL。这包括混合细胞腺瘤、嗜酸性干细胞来源的腺瘤、催乳生长素细胞来源的腺瘤以及仅分泌 GH 的大腺瘤压迫垂体柄。[14]Bonert VS, Melmed S. Acromegaly with moderate hyperprolactinemia caused by an intrasellar macroadenoma. Nat Clin Pract Endocrinol Metab. 2006 Jul;2(7):408-12.http://www.ncbi.nlm.nih.gov/pubmed/16932323?tool=bestpractice.com 这些肿瘤或存在共分泌GH和PRL的细胞,或存在两种不同细胞群(一种分泌GH,另外一种分泌PRL),可同时引起肢端肥大症和高泌乳素血症。
影响垂体的非肿瘤性疾病
垂体柄创伤性截断。
淋巴细胞性垂体炎是由垂体自身免疫性疾病伴淋巴细胞浸润引起的。这种情况通常发生在妊娠末期或产后早期,但不绝对是这样。患者通常还存在其他自身免疫性疾病,例如,自身免疫性甲状腺疾病(主要是桥本氏甲状腺炎)、Addison 病、1 型糖尿病、甲状旁腺功能减退症和自身免疫性肝炎。这也可能是自身免疫性多内分泌腺病综合征的一部分。[1]Casanueva FF, Molitch ME, Schlechte JA, et al. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf). 2006 Aug;65(2):265-73.https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2265.2006.02562.xhttp://www.ncbi.nlm.nih.gov/pubmed/16886971?tool=bestpractice.com[2]Serri O, Chik CL, Ur E, et al. Diagnosis and management of hyperprolactinemia. CMAJ. 2003 Sep 16;169(6):575-81.http://www.cmaj.ca/content/169/6/575.longhttp://www.ncbi.nlm.nih.gov/pubmed/12975226?tool=bestpractice.com[15]Beressi N, Beressi JP, Cohen R, et al. Lymphocytic hypophysitis. A review of 145 cases. Ann Med Interne (Paris). 1999 Jun;150(4):327-41.http://www.ncbi.nlm.nih.gov/pubmed/10519020?tool=bestpractice.com
肉芽肿性垂体炎是由结节病或其他肉芽肿性疾病(如结核病、梅毒、组织细胞增生症 X 及特发性肉芽肿性垂体炎)引起的。[16]Bhardwaj M, Sharma A, Pal HK. Granulomatous hypophysitis. Neurol India. 2005 Sep;53(3):364-5.http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2005;volume=53;issue=3;spage=364;epage=365;aulast=Bhardwajhttp://www.ncbi.nlm.nih.gov/pubmed/16230818?tool=bestpractice.com
原发性甲状腺功能减退症
该病在 8% 的病例中可引起 PRL 水平轻度升高 (<2174 pmol/L [50 μg/L])。[17]Cortet-Rudelli C, Sapin R, Bonneville JF, et al. Etiological diagnosis of hyperprolactinemia. Ann Endocrinol (Paris). 2007 Jun;68(2-3):98-105.http://www.ncbi.nlm.nih.gov/pubmed/17524347?tool=bestpractice.com 甲状腺激素替代治疗可使PRL水平恢复正常。
在存在甲状腺相关问题的连续患者系列中,有 21% 的显性甲状腺功能减退的患者出现 PRL 水平升高,在亚临床型甲状腺功能减退症患者中,有 8% 的患者发生 PRL 水平升高。[18]Goel P, Kahkasha, Narang S, et al. Evaluation of serum prolactin level in patients of subclinical and overt hypothyroidism. J Clin Diagn Res. 2015 Jan;9(1):BC15-7.https://www.jcdr.net/article_fulltext.asp?issn=0973-709x&year=2015&volume=9&issue=1&page=BC15&issn=0973-709x&id=5443http://www.ncbi.nlm.nih.gov/pubmed/25737975?tool=bestpractice.com
甲状腺功能减退也与促甲状腺激素细胞(以及泌乳素细胞)增生有关,会导致明显的垂体增大。 在影像学上容易与催乳素瘤混淆。
多发性内分泌腺瘤综合征I型
催乳素瘤可能是该综合征中的一种表现,并与其他内分泌肿瘤有关,比如,甲状旁腺肿瘤、胰腺肿瘤(胰岛瘤、胃泌素瘤)或者肾上腺腺瘤。[1]Casanueva FF, Molitch ME, Schlechte JA, et al. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf). 2006 Aug;65(2):265-73.https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2265.2006.02562.xhttp://www.ncbi.nlm.nih.gov/pubmed/16886971?tool=bestpractice.com
多囊卵巢综合征 (PCOS)
高泌乳素血症(伴有 PRL 水平<2174 pmol/L [50 μg/L]),[17]Cortet-Rudelli C, Sapin R, Bonneville JF, et al. Etiological diagnosis of hyperprolactinemia. Ann Endocrinol (Paris). 2007 Jun;68(2-3):98-105.http://www.ncbi.nlm.nih.gov/pubmed/17524347?tool=bestpractice.com 估计 14.7% 的 PCOS 患者会发生高催乳素血症,但尚不清楚与此相关的病理生理机制。根据一项研究,PCOS 女性患者的 PRL 浓度>85.2ng/mL 高度提示催乳素瘤(敏感性为 77%,特异性为 100%)。[19]Kyritsi EM, Dimitriadis GK, Angelousi A, et al. The value of prolactin in predicting prolactinοma in hyperprolactinaemic polycystic ovarian syndrome. Eur J Clin Invest. 2018 Jul;48(7):e12961.http://www.ncbi.nlm.nih.gov/pubmed/29845629?tool=bestpractice.com
慢性肾功能衰竭
肝硬化
20%的肝硬化患者可出现基础PRL水平增高。[1]Casanueva FF, Molitch ME, Schlechte JA, et al. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf). 2006 Aug;65(2):265-73.https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2265.2006.02562.xhttp://www.ncbi.nlm.nih.gov/pubmed/16886971?tool=bestpractice.com[2]Serri O, Chik CL, Ur E, et al. Diagnosis and management of hyperprolactinemia. CMAJ. 2003 Sep 16;169(6):575-81.http://www.cmaj.ca/content/169/6/575.longhttp://www.ncbi.nlm.nih.gov/pubmed/12975226?tool=bestpractice.com[3]Mah PM, Webster J. Hyperprolactinemia: etiology, diagnosis, and management. Semin Reprod Med. 2002 Nov;20(4):365-74.http://www.ncbi.nlm.nih.gov/pubmed/12536359?tool=bestpractice.com
胸壁创伤或手术
通过乳腺神经介导的反射导致高泌乳素血症。[1]Casanueva FF, Molitch ME, Schlechte JA, et al. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf). 2006 Aug;65(2):265-73.https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2265.2006.02562.xhttp://www.ncbi.nlm.nih.gov/pubmed/16886971?tool=bestpractice.com[2]Serri O, Chik CL, Ur E, et al. Diagnosis and management of hyperprolactinemia. CMAJ. 2003 Sep 16;169(6):575-81.http://www.cmaj.ca/content/169/6/575.longhttp://www.ncbi.nlm.nih.gov/pubmed/12975226?tool=bestpractice.com[3]Mah PM, Webster J. Hyperprolactinemia: etiology, diagnosis, and management. Semin Reprod Med. 2002 Nov;20(4):365-74.http://www.ncbi.nlm.nih.gov/pubmed/12536359?tool=bestpractice.com 这种反射也是导致与特发性肉芽肿性乳腺炎相关的高催乳素血症的机制。[20]Pluguez-Turull CW, Nanyes JE, Quintero CJ, et al. Idiopathic granulomatous mastitis: manifestations at multimodality imaging and pitfalls. Radiographics. 2018 Mar-Apr;38(2):330-56.http://www.ncbi.nlm.nih.gov/pubmed/29528819?tool=bestpractice.com
异位高泌乳素血症
这种疾病是一种副癌表现,PRL 由来源于垂体腺之外组织的肿瘤产生,例如卵巢或间叶细胞(血管周上皮样细胞)肿瘤。[21]Kallenberg GA, Pesce CM, Norman B, et al. Ectopic hyperprolactinemia resulting from an ovarian teratoma. JAMA. 1990 May 9;263(18):2472-4.http://www.ncbi.nlm.nih.gov/pubmed/2329635?tool=bestpractice.com[22]Korytnaya E, Liu J, Camelo-Piragua S, et al. Ectopic prolactin secretion from a perivascular epithelioid cell tumor (PEComa). J Clin Endocrinol Metab. 2014 Nov;99(11):3960-4.http://www.ncbi.nlm.nih.gov/pubmed/25127092?tool=bestpractice.com
外科手术切除产生PRL的肿瘤能够使PRL水平恢复正常。
药理学因素
药物诱发的高催乳素血症通常 PRL 水平<4348 pmol/L (100 μg/L)。
抗精神病药物(吩噻嗪类、噻吨、丁酰苯和非典型抗精神病药物)是药物诱发高泌乳素血症的最常见原因。在服用这些药物(也称精神安定剂)的患者中,约有60%的女性和40%的男性会出现高泌乳素血症。[23]Haddad PM, Wieck A. Antipsychotic-induced hyperprolactinemia: mechanisms, clinical features and management. Drugs. 2004;64(20):2291-314.http://www.ncbi.nlm.nih.gov/pubmed/15456328?tool=bestpractice.com
尽管第一代抗精神病药物引起PRL水平增高最高,但第二代抗精神病药物也可导致高泌乳素血症。 据报道,阿米舒必利、利培酮和帕潘立酮具有最高的发生率。(即使低剂量也可增高PRL),而阿立哌唑和喹硫平对PRL 水平影响最小。 治疗开始后PRL水平通常增高,呈剂量依赖性。 阿立哌唑甚至可以降低PRL水平。[24]Peuskens J, Pani L, Detraux J, et al. The effects of novel and newly approved antipsychotics on serum prolactin levels: a comprehensive review. CNS Drugs. 2014 May;28(5):421-53.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4022988/http://www.ncbi.nlm.nih.gov/pubmed/24677189?tool=bestpractice.com
其他可引起高泌乳素血症的药物包括:[25]Molitch ME. Medication-induced hyperprolactinemia. Mayo Clin Proc. 2005 Aug;80(8):1050-7.https://www.mayoclinicproceedings.org/article/S0025-6196(11)61587-5/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/16092584?tool=bestpractice.com[26]Teoh SK, Lex BW, Mendelson JH, et al. Hyperprolactinemia and macrocytosis in women with alcohol and polysubstance dependence. J Stud Alcohol. 1992 Mar;53(2):176-82.http://www.ncbi.nlm.nih.gov/pubmed/1560669?tool=bestpractice.com[27]Coker F, Taylor D. Antidepressant-induced hyperprolactinaemia: incidence, mechanisms and management. CNS Drugs. 2010 Jul;24(7):563-74.http://www.ncbi.nlm.nih.gov/pubmed/20527996?tool=bestpractice.com[28]Madhusoodanan S, Parida S, Jimenez C. Hyperprolactinemia associated with psychotropics: a review. Hum Psychopharmacol. 2010 Jun-Jul;25(4):281-97.http://www.ncbi.nlm.nih.gov/pubmed/20521318?tool=bestpractice.com[29]Sarkar DK. Hyperprolactinemia following chronic alcohol administration. Front Horm Res. 2010;38:32-41.http://www.ncbi.nlm.nih.gov/pubmed/20616493?tool=bestpractice.com
多巴胺受体阻滞剂(胃复安、多潘立酮、利培酮、吩噻嗪类三环类抗抑郁药、西咪替丁)
干扰多巴胺合成或存储的药物(例如:甲基多巴、单胺氧化酶抑制剂 [MAOI])[25]Molitch ME. Medication-induced hyperprolactinemia. Mayo Clin Proc. 2005 Aug;80(8):1050-7.https://www.mayoclinicproceedings.org/article/S0025-6196(11)61587-5/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/16092584?tool=bestpractice.com
抗抑郁药物(三环和四环类抗抑郁药、单胺氧化酶抑制剂、5-羟色胺再吸收抑制剂、奈法唑酮、安非他酮和文拉法辛)
阿片和可卡因
降压药(例如:维拉帕米、甲基多巴)
胃肠道药物[甲氧氯普胺、多潘立酮、组胺受体 (H2) 阻滞剂、蛋白酶抑制剂(部分研究结果不一致)]
雌二醇
酒精(摄入过量)。
生理学
巨泌乳素血症
高水平巨泌乳素导致PRL-IgG 复合物清除率降低。
巨泌乳素血症在高泌乳素血症中的发生率为15%~46%。[1]Casanueva FF, Molitch ME, Schlechte JA, et al. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf). 2006 Aug;65(2):265-73.https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2265.2006.02562.xhttp://www.ncbi.nlm.nih.gov/pubmed/16886971?tool=bestpractice.com[5]Gibney J, Smith TP, McKenna TJ. Clinical relevance of macroprolactin. Clin Endocrinol (Oxf). 2005 Jun;62(6):633-43.https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2265.2005.02243.xhttp://www.ncbi.nlm.nih.gov/pubmed/15943822?tool=bestpractice.com[17]Cortet-Rudelli C, Sapin R, Bonneville JF, et al. Etiological diagnosis of hyperprolactinemia. Ann Endocrinol (Paris). 2007 Jun;68(2-3):98-105.http://www.ncbi.nlm.nih.gov/pubmed/17524347?tool=bestpractice.com
在普通人群中,据估计发生率女性0.2%和男性0.02%。
好发于特发性高泌乳素血症,在与特发性高泌乳素相关疾病如抗精神病药物诱发的高泌乳素血症中也有报道。[30]De Schepper J, Schiettecatte J, Velkeniers B, et al. Clinical and biological characterization of macroprolactinemia with and without prolactin-IgG complexes. Eur J Endocrinol. 2003 Sep;149(3):201-7.https://eje.bioscientifica.com/view/journals/eje/149/3/201.xmlhttp://www.ncbi.nlm.nih.gov/pubmed/12943522?tool=bestpractice.com
系统性红斑狼疮患者中40%可存在巨泌乳素血症,可能由于存在抗PRL自身抗体。[31]Leanos A, Pascoe D, Fraga A, et al. Anti-prolactin autoantibodies in systemic lupus erythematosus patients with associated hyperprolactinemia. Lupus. 1998;7(6):398-403.http://www.ncbi.nlm.nih.gov/pubmed/9736323?tool=bestpractice.com
当高泌乳素血症患者缺乏典型症状和/或缺乏垂体瘤影像学证据时,应怀疑存在巨泌乳素血症。 然而,一项纳入106例患者的研究报道了在这些患者中出现闭经、溢乳和/或不孕。[32]Vallette-Kasic S, Morange-Ramos I, Selim A, et al. Macroprolactinemia revisited: a study on 106 patients. J Clin Endocrinol Metab. 2002 Feb;87(2):581-8.https://academic.oup.com/jcem/article/87/2/581/2846759http://www.ncbi.nlm.nih.gov/pubmed/11836289?tool=bestpractice.com
PRL 水平通常<4348 pmol/L (100 μg/L),只有 8.5% 到 20% 的患者 PRL 水平达到 4348 pmol/L (100 μg/L)。[17]Cortet-Rudelli C, Sapin R, Bonneville JF, et al. Etiological diagnosis of hyperprolactinemia. Ann Endocrinol (Paris). 2007 Jun;68(2-3):98-105.http://www.ncbi.nlm.nih.gov/pubmed/17524347?tool=bestpractice.com[32]Vallette-Kasic S, Morange-Ramos I, Selim A, et al. Macroprolactinemia revisited: a study on 106 patients. J Clin Endocrinol Metab. 2002 Feb;87(2):581-8.https://academic.oup.com/jcem/article/87/2/581/2846759http://www.ncbi.nlm.nih.gov/pubmed/11836289?tool=bestpractice.com
生理应激
妊娠、哺乳、刺激乳头
妊娠期间,雌激素浓度上升通过刺激泌乳素细胞导致 PRL 水平增高。在妊娠期间观察到泌乳素细胞变大且数量增多。然而,高水平的雌激素和孕激素在妊娠期抑制泌乳,产后雌激素和孕激素水平下降,引起泌乳。[33]Saleem M, Martin H, Coates P. Prolactin biology and laboratory measurement: an update on physiology and current analytical issues. Clin Biochem Rev. 2018 Feb;39(1):3-16.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6069739/http://www.ncbi.nlm.nih.gov/pubmed/30072818?tool=bestpractice.com
乳头刺激通过乳腺神经介导的反射导致高泌乳素血症。
其他生理性病因包括:
运动、进食、性交、睡眠和心理压力。[33]Saleem M, Martin H, Coates P. Prolactin biology and laboratory measurement: an update on physiology and current analytical issues. Clin Biochem Rev. 2018 Feb;39(1):3-16.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6069739/http://www.ncbi.nlm.nih.gov/pubmed/30072818?tool=bestpractice.com
特发性
罕见情况下,高催乳素血症(通常达到 4348 pmol/L [100 μg/L] 的水平)的潜在原因无法明确,因此将这种疾病称为特发性高催乳素血症。[1]Casanueva FF, Molitch ME, Schlechte JA, et al. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf). 2006 Aug;65(2):265-73.https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2265.2006.02562.xhttp://www.ncbi.nlm.nih.gov/pubmed/16886971?tool=bestpractice.com[2]Serri O, Chik CL, Ur E, et al. Diagnosis and management of hyperprolactinemia. CMAJ. 2003 Sep 16;169(6):575-81.http://www.cmaj.ca/content/169/6/575.longhttp://www.ncbi.nlm.nih.gov/pubmed/12975226?tool=bestpractice.com[3]Mah PM, Webster J. Hyperprolactinemia: etiology, diagnosis, and management. Semin Reprod Med. 2002 Nov;20(4):365-74.http://www.ncbi.nlm.nih.gov/pubmed/12536359?tool=bestpractice.com
这种患者可能存在计算机体层成像和磁共振成像不能发现的微腺瘤。[34]Hattori N, Ishihara T, Ikekubo K, et al. Autoantibody to human prolactin in patients with idiopathic hyperprolactinemia. J Clin Endocrinol Metab. 1992 Nov;75(5):1226-9.http://www.ncbi.nlm.nih.gov/pubmed/1430082?tool=bestpractice.com 在不存在自身免疫性疾病情况下,约16%的特发性高泌乳素血症患者可检测出抗PRL自身抗体。[34]Hattori N, Ishihara T, Ikekubo K, et al. Autoantibody to human prolactin in patients with idiopathic hyperprolactinemia. J Clin Endocrinol Metab. 1992 Nov;75(5):1226-9.http://www.ncbi.nlm.nih.gov/pubmed/1430082?tool=bestpractice.com[35]Hattori N, Ikekubo K, Ishihara T, et al. Effects of anti-prolactin autoantibodies on serum prolactin measurements. Eur J Endocrinol. 1994 May;130(5):434-7.http://www.ncbi.nlm.nih.gov/pubmed/8180668?tool=bestpractice.com
