参见 鉴别诊断 以获取更多具体信息
所有病重或恶化的患者都应遵循气道、呼吸、循环、神经损伤、全身检查 (ABCDE) 方法进行评估。[5]Resuscitation Council (UK). Reuscitation guidelines: the ABCDE approach. 2015 [internet publication].https://www.resus.org.uk/resuscitation-guidelines/abcde-approach/ 对于任何一个呼吸困难的患者,临床医生应迅速评估气道状态,采取必要措施确保气道通畅。 例如摆正体位,和/或保持鼻腔或口腔通畅。
 鼻咽气道的动画演示
鼻咽气道的动画演示
 口咽气道的动画演示
口咽气道的动画演示
对于极度呼吸困难患者,建议及时咨询麻醉科医师进行评估。 应进行脉搏血氧测定或动脉血气检测以评估氧和情况,并且若需要的话应采取辅助供氧。如果患者极度不适,应首先给予高流量氧,然后等待进一步检查。英国胸科协会指南建议,一旦能够使用可靠的脉搏血氧测定法,就应对大多数急性患者或具有高碳酸性呼吸衰竭风险的患者使用氧气,以使前者达到 94% 至 98% 的目标血氧饱和度,使后者达到 88% 至 92% 的目标血氧饱和度(或患者特定的目标范围)。[8]O'Driscoll BR, Howard LS, Earis J, et al; British Thoracic Society Emergency Oxygen Guideline Group; BTS Emergency Oxygen Guideline Development Group. BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax. 2017;72(suppl 1):ii1-90.https://www.brit-thoracic.org.uk/document-library/clinical-information/oxygen/2017-emergency-oxygen-guideline/bts-guideline-for-oxygen-use-in-adults-in-healthcare-and-emergency-settings/http://www.ncbi.nlm.nih.gov/pubmed/28507176?tool=bestpractice.com在不同组织对于特定疾病的指南中,关于辅助供氧和目标范围所给建议可能有所不同。一项系统评价和 meta 分析发现,与保守用氧方式相比,大量用氧可增加急性患者的死亡率。[9]Siemieniuk RAC, Chu DK, Kim LH, et al. Oxygen therapy for acutely ill medical patients: a clinical practice guideline. BMJ. 2018 Oct 24;363:k4169.https://www.bmj.com/content/363/bmj.k4169http://www.ncbi.nlm.nih.gov/pubmed/30355567?tool=bestpractice.com[10]Chu DK, Kim LH, Young PJ, et al. Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis. Lancet. 2018 Apr 28;391(10131):1693-705.http://www.ncbi.nlm.nih.gov/pubmed/29726345?tool=bestpractice.com
应对突发重度呼吸困难或静息时呼吸困难的患者针对其胸痛进行询问,并确定患者是否有冠状动脉病变、充血性心力衰竭、慢性阻塞性肺疾病 (COPD) 或哮喘的病史。
对问题的初步反应、ABCDE 检查的结果及临床观察有助于确认最有可能的诊断结果,然后可根据最有可能的诊断结果确定紧急的进一步检查和治疗。
急性冠脉综合征 (ACS)
一般表现为心前区疼痛放射至肩部、颈部,常伴有呼吸困难。但是,在女性、糖尿病患者和年龄在 75 岁及以上的患者中,可有不典型的表现,例如仅有呼吸困难而无疼痛、或者有不典型疼痛。[11]Brieger D, Eagle KA, Goodman SG, et al. Acute coronary syndromes without chest pain, an underdiagnosed and undertreated high-risk group: insights from the Global Registry of Acute Coronary Events. Chest. 2004 Aug;126(2):461-9.http://www.ncbi.nlm.nih.gov/pubmed/15302732?tool=bestpractice.com[12]Canto JG, Goldberg RJ, Hand MM, et al. Symptom presentation of women with acute coronary syndromes: myth vs reality. Arch Intern Med. 2007 Dec 10;167(22):2405-13.http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/770038http://www.ncbi.nlm.nih.gov/pubmed/18071161?tool=bestpractice.com[13]Jacoby RM, Nesto RW. Acute myocardial infarction in the diabetic patient: pathophysiology, clinical course and prognosis. J Am Coll Cardiol. 1992 Sep;20(3):736-44.http://www.ncbi.nlm.nih.gov/pubmed/1512357?tool=bestpractice.com伴有急性冠状动脉病变的呼吸困难预后较差。[14]Abidov A, Rozanski A, Hachamovitch R, et al. Prognostic significance of dyspnea in patients referred for cardiac stress testing. N Engl J Med. 2005 Nov 3;353(18):1889-98.http://www.nejm.org/doi/full/10.1056/NEJMoa042741#t=articlehttp://www.ncbi.nlm.nih.gov/pubmed/16267320?tool=bestpractice.com
患者可出现皮肤湿冷及低血压。心脏听诊可闻及第三或第四心音奔马律,肺部听诊可闻及罗音。存在特征性心电图改变,并伴随心肌损伤的生化证据(心肌酶升高),有助于确诊。[15]O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013 Jan 29;127(4):e362-425.http://circ.ahajournals.org/content/127/4/e362.longhttp://www.ncbi.nlm.nih.gov/pubmed/23247304?tool=bestpractice.com[16]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014 Dec 23;130(25):e344-426.http://circ.ahajournals.org/content/130/25/e344.longhttp://www.ncbi.nlm.nih.gov/pubmed/25249585?tool=bestpractice.comACS 分为以下三种临床类型:
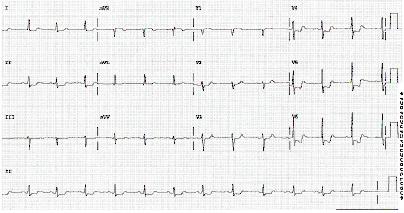
ST 段抬高型心肌梗死 (STEMI):心电图 (ECG) 显示在两个或以上的解剖部位相邻导联有 ST 段持续抬高,或新发左束支传导阻滞。
 [Figure caption and citation for the preceding image starts]: 12导联心电图显示下壁和前壁导联ST段抬高,侧壁导联呈对应性改变来源于 Mahi Ashwath 医生的个人收集;获得允许后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 12导联心电图显示下壁和前壁导联ST段抬高,侧壁导联呈对应性改变来源于 Mahi Ashwath 医生的个人收集;获得允许后使用 [Citation ends].
非 ST 段抬高型心肌梗死 (NSTEMI):心电图未显示 ST 段抬高,但是心脏生物标志物水平升高。心电图可能显示非特异性缺血改变,例如 ST 段压低或 T 波倒置。
 [Figure caption and citation for the preceding image starts]: 心电图显示 ST 段压低来源:休斯顿德克萨斯大学心内科医生 Syed W. Yusuf 博士和 Iyad N. Daher 博士;经允许后使用。 [Citation ends].
[Figure caption and citation for the preceding image starts]: 心电图显示 ST 段压低来源:休斯顿德克萨斯大学心内科医生 Syed W. Yusuf 博士和 Iyad N. Daher 博士;经允许后使用。 [Citation ends].
3.不稳定型心绞痛:心电图非特异性缺血改变,但是心脏生物标记物正常。
及时的临床和心电图评估是诊断急性冠脉综合征的关键。
在 STEMI 患者中,立即行血流重建(经皮冠状动脉介入治疗或纤溶疗法)可改善生存率。阿司匹林和其他抗血小板药物、β 受体阻滞剂、硝酸酯类药物和抗凝血药被用作不同形式的 ACS 的初始治疗。
急性哮喘
突发呼吸困难(尤其是在有既往哮喘病史者当中)可能提示急性哮喘发作。可能伴有逐渐加重的喘息和咳嗽,但是在重症患者中也可能不发生喘息。根据英国胸科协会 (British Thoracic Society, BTS) 指南的定义,出现下述任一特征即为急性重度哮喘:最佳或预测呼气流量峰值为 33% 至 50%、呼吸频率≥25 次/分、心率≥110 次/分、无法一口气说完句子。[17]British Thoracic Society, Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma. A national clinical guideline. September 2016 [internet publication].http://www.sign.ac.uk/assets/sign153.pdf 在重度致敏情况下,接触气源性过敏源(例如猫毛屑)可诱发哮喘发作。突发重度哮喘、气管插管和机械通气、频繁急诊就诊、重症监护病房治疗、吸入大剂量支气管扩张剂、目前使用或停用皮质类固醇者的既往史是重度哮喘发作的标志,也是危及生命发作的预测因子。初始治疗是使用高剂量的吸入性 β-2 受体激动剂支气管舒张剂,或含抗胆碱能的 β-2 受体激动剂、[18]Kirkland SW, Vandenberghe C, Voaklander B, et al. Combined inhaled beta-agonist and anticholinergic agents for emergency management in adults with asthma. Cochrane Database Syst Rev. 2017;(1):CD001284.http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD001284.pub2/fullhttp://www.ncbi.nlm.nih.gov/pubmed/28076656?tool=bestpractice.com [  ]How does an anticholinergic agent added to an inhaled short-acting beta-agonist (SABA) compare with SABA alone for emergency management of asthma in adults?https://cochranelibrary.com/cca/doi/10.1002/cca.1826/full显示答案皮质类固醇(剂量充足)、有时插管行机械通气。[17]British Thoracic Society, Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma. A national clinical guideline. September 2016 [internet publication].http://www.sign.ac.uk/assets/sign153.pdf
]How does an anticholinergic agent added to an inhaled short-acting beta-agonist (SABA) compare with SABA alone for emergency management of asthma in adults?https://cochranelibrary.com/cca/doi/10.1002/cca.1826/full显示答案皮质类固醇(剂量充足)、有时插管行机械通气。[17]British Thoracic Society, Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma. A national clinical guideline. September 2016 [internet publication].http://www.sign.ac.uk/assets/sign153.pdf
出现急性哮踹的患者需要立即接受治疗。根据以下要素决定对紧急就诊但未诊断哮踹的患者进行客观性检查的时机:检查的可及性,以及检查是否会削弱急性治疗的效果。[19]National Institute for Health and Care Excellence. Asthma: diagnosis, monitoring and chronic asthma management. November 2017 [internet publication].https://www.nice.org.uk/guidance/ng80 通常情况下,根据结构化的临床评估进行哮喘诊断。该项评估包括典型病史(在夜间和接触变应原、寒冷环境或烟雾而加重的阵发性呼吸困难和喘息;慢性咳嗽)、既往病史回顾、证实气流阻塞和可逆性。[17]British Thoracic Society, Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma. A national clinical guideline. September 2016 [internet publication].http://www.sign.ac.uk/assets/sign153.pdf[20]Global Initiative for Asthma. 2018 GINA report: global strategy for asthma management and prevention. March 2018 [internet publication].https://ginasthma.org/wp-content/uploads/2018/04/wms-GINA-2018-report-V1.3-002.pdf2017 年英国国家卫生与临床优化研究所 (NICE) 哮踹指南建议,对于可能患有哮踹的17岁及以上成人,若有条件,应在进行肺量测定前,先进行呼出气一氧化氮 (FeNO) 检测。FeNO 水平>40 ppb 应视为阳性。[19]National Institute for Health and Care Excellence. Asthma: diagnosis, monitoring and chronic asthma management. November 2017 [internet publication].https://www.nice.org.uk/guidance/ng80 进一步检查包括支气管激发试验。
重度慢性阻塞性肺病急性加重 (COPD)
COPD 急性加重通常表现为呼吸困难水平加重、慢性咳嗽加重和/或痰量增多和/或痰液呈脓性。使用辅助呼吸肌、反常呼吸、发绀、新发外周水肿、血流动力学不稳定和/或精神状态恶化(例如,意识模糊、嗜睡、昏迷)是严重程度恶化的重要指标。发生威胁生命的加重患者需要在重症监护病房内接受治疗。
对于严重但无生命危险的症状加重患者,其初始治疗包括:联用短效 β-2 受体激动剂和短效抗胆碱能药物、在患者缺氧时辅助供氧(但供氧时应小心谨慎,防止进一步的高碳酸血症)、全身皮质类固醇治疗,以及在疑似发生细菌感染时使用抗生素。对于初始治疗反应不佳的重度急性加重患者应该进行无创通气 (NIV) 治疗。在无禁忌证的情况下,建议将 NIV 作为急性呼吸衰竭和慢性阻塞性肺疾病 (COPD) 患者的首选通气疗法。[21]Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease: 2019 report. 2019 [internet publication].https://goldcopd.org/gold-reports/ 《慢性阻塞性肺疾病全球倡议》(GOLD) 2019 年报告中提到了针对 COPD 急性加重患者的无创通气和有创通气的适应症。[21]Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease: 2019 report. 2019 [internet publication].https://goldcopd.org/gold-reports/
过敏反应
易感人群接触药物、食物或蚊虫叮咬后,可出现全身过敏性反应、 突发呼吸困难、皮肤病变(皮疹、瘙痒、荨麻疹和血管性水肿)、声音嘶哑、窒息感、舌及颜面部水肿、喘息、心动过速及低血压。 有时表现为恶心、呕吐和腹泻。
其诊断依赖临床。急救治疗措施可挽救生命,包括:及时去除刺激性抗原、在诊断出严重过敏反应后立即在股前外侧肌内注射肾上腺素、气道管理及容量复苏。[22]Campbell RL, Li JT, Nicklas RA, et al; members of the Joint Task Force; Practice Parameter Workgroup. Emergency department diagnosis and treatment of anaphylaxis: a practice parameter. Ann Allergy Asthma Immunol. 2014 Dec;113(6):599-608.http://www.annallergy.org/article/S1081-1206(14)00743-1/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/25466802?tool=bestpractice.com
误吸异物
癫痫、晕厥、心理状态改变(如中毒、低血糖等)、窒息和进食后咳嗽(特别是坚果)者,常提示吸食异物。 若气道狭小(如在儿童和青少年),异物位于下咽部或声门处,可导致窒息、危及生命。
随后可出现发绀和喘鸣,然后是低血压和循环衰竭。有意识的成人和儿童的初始处理方式包括掌击背部,以及若该方法未成功则行腹部冲击(海姆立克急救法)。对于有意识的婴儿,推荐先掌击背部,随后行胸部冲击;不要对婴儿实施腹部冲击。[23]Monsieurs KG, Nolan JP, Bossaert LL, et al; ERC Guidelines 2015 Writing Group. European Resuscitation Council guidelines for resuscitation 2015: Section 1. Executive summary. Resuscitation. 2015 Oct;95:1-80.https://www.resuscitationjournal.com/article/S0300-9572(15)00350-0/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/26477410?tool=bestpractice.com在具有医疗条件的环境中,可尝试移除异物,同时经口气管插管或环甲膜切开术可提供紧急气道处理。
肺癌
咳嗽是肺癌的最常见症状,可能伴有体重减轻、咯血、胸痛、呼吸困难或声嘶。有吸烟史或正在吸烟是导致肺癌的最大危险因素。影像学和病理学结果可明确肺癌诊断,肺癌的治疗方法包括手术、化疗和放疗。需要紧急处理的急性表现包括大量咯血、阻塞性肺炎/缺氧和上腔静脉综合征。应立即让出现大量咯血的患者维持一个体位,使得推测出血的肺(如已知)位于下垂位。可能需要对未出血的主支气管进行选择性插管或进行双腔插管以保护气道。软式支气管镜检查或动脉造影技术可用于明确控制出血。[24]Radchenko C, Alraiyes AH, Shojaee S. A systematic approach to the management of massive hemoptysis. J Thorac Dis. 2017 Sep;9(suppl 10):S1069-86.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5696556/http://www.ncbi.nlm.nih.gov/pubmed/29214066?tool=bestpractice.com
对于由近侧肺部肿瘤引起的阻塞性肺炎,可采用下列方法进行初始治疗:保护气道,然后施行一系列局部(介入性或硬质支气管镜检查)或外部(外放疗)治疗方法。[25]Simoff MJ, Lally B, Slade MG, et al. Symptom management in patients with lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(suppl 5):e455S-97S.http://journal.chestnet.org/article/S0012-3692(13)60305-0/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/23649452?tool=bestpractice.com
由恶性梗阻引起的上腔静脉综合征可通过放置静脉支架或放射疗法进行初始处理。[25]Simoff MJ, Lally B, Slade MG, et al. Symptom management in patients with lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(suppl 5):e455S-97S.http://journal.chestnet.org/article/S0012-3692(13)60305-0/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/23649452?tool=bestpractice.com
上气道梗阻
可能因异物、气道肿瘤(舌根部、喉部、食管及气管)、水肿、上呼吸道结构功能障碍(例如声带功能障碍、血管性水肿)和外源性压迫(例如声门下狭窄、胸骨后甲状腺肿、淋巴瘤)。
通常表现为显著的呼吸困难,吸气性喘鸣,偶有呼气性喘鸣,运动诱导的气流增加可加剧上述表现。
紧急处理包括开放气道,通过影像技术和支气管镜检查明确病因及治疗。
严重肺炎
肺炎的临床诊断依据是一组与下呼吸道感染相关的体征和症状且伴有呼吸困难、发热>38ºC (>100ºF)、咳嗽、咳痰、胸痛和肺泡腔浸润的体征。需要特别注意的是,老年患者通常无发热,但可能出现意识模糊和基础疾病恶化。存在各种用于评估严重程度的计分系统,包括肺炎严重程度指数 (pneumonia severity index, PSI)[26]Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997 Jan 23;336(4):243-50.http://www.nejm.org/doi/full/10.1056/NEJM199701233360402http://www.ncbi.nlm.nih.gov/pubmed/8995086?tool=bestpractice.com 和针对社区获得性肺炎 (community-acquired pneumonia, CAP) 的 CURB-65,[27]Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003 May;58(5):377-82.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1746657/pdf/v058p00377.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/12728155?tool=bestpractice.com 且得分随死亡率的增加而增高。
指南推荐对怀疑 CAP 的患者在出现下列情况时进行住院治疗:[28]Lim WS, Baudouin SV, George RC, et al; Pneumonia Guidelines Committee of the BTS Standards of Care Committee. British Thoracic Society guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax. 2009 Oct;64(suppl 3):iii1-55.http://thorax.bmj.com/content/64/Suppl_3/iii1.longhttp://www.ncbi.nlm.nih.gov/pubmed/19783532?tool=bestpractice.com[29]Mandell LA, Wunderink RG, Anzueto A, et al; Infectious Diseases Society of America; American Thoracic Society. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007 Mar 1;44(suppl 2):S27-72.https://academic.oup.com/cid/article/44/Supplement_2/S27/372079http://www.ncbi.nlm.nih.gov/pubmed/17278083?tool=bestpractice.com
PSI 评分为 71 至 90 分的患者(III 级;短期住院可能给患者带来益处)
PSI 评分为 91 至 130 分(IV 级)或评分>130 分的患者(V 级;死亡风险分别为 9% 和 27%)。[26]Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med. 1997 Jan 23;336(4):243-50.http://www.nejm.org/doi/full/10.1056/NEJM199701233360402http://www.ncbi.nlm.nih.gov/pubmed/8995086?tool=bestpractice.com
CURB-65 评分≥3 分以及评分为 4 分或 5 分的患者(预期死亡率分别为 15% 至 40%,并且应考虑收入重症监护病房)
所有表现为低氧血症(SaO2 <90% 或 PaO2 <60 mmHg)或严重血流动力学不稳定的患者(这些患者无论其严重度评分如何,均应收治入院)
因高风险致病菌罹患 CAP 或伴有化脓性或转移性疾病的患者。[30]Halm EA, Teirstein AS. Clinical practice. Management of community-acquired pneumonia. N Engl J Med. 2002 Dec 19;347(25):2039-45.http://www.ncbi.nlm.nih.gov/pubmed/12490686?tool=bestpractice.com
住院治疗的患者应接受恰当的氧疗,同时监测血氧饱和度和吸氧浓度,目标将 SaO2 维持在 94% 以上。对于并发通气衰竭的 COPD 患者,应根据重复测量的动脉血气水平以指导氧疗。[28]Lim WS, Baudouin SV, George RC, et al; Pneumonia Guidelines Committee of the BTS Standards of Care Committee. British Thoracic Society guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax. 2009 Oct;64(suppl 3):iii1-55.http://thorax.bmj.com/content/64/Suppl_3/iii1.longhttp://www.ncbi.nlm.nih.gov/pubmed/19783532?tool=bestpractice.com 尽管经过了适当的氧治疗,呼吸衰竭患者仍需要进行紧急气道管理和(有可能)插管。应评估患者容量减少的情况,并应根据需要进行静脉输液。对于患有长期疾病的患者应提供营养支持。[28]Lim WS, Baudouin SV, George RC, et al; Pneumonia Guidelines Committee of the BTS Standards of Care Committee. British Thoracic Society guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax. 2009 Oct;64(suppl 3):iii1-55.http://thorax.bmj.com/content/64/Suppl_3/iii1.longhttp://www.ncbi.nlm.nih.gov/pubmed/19783532?tool=bestpractice.com 初始社区获得性肺炎的经验性抗生素治疗应遵循国际指南及当地流行病学现状。重要的是考虑脓毒症的可能性,因为及早识别和治疗可改善治疗结局。[31]National Institute for Health and Care Excellence. Sepsis: recognition, diagnosis and early management. September 2017 [internet publication].https://www.nice.org.uk/guidance/ng51[32]Gao F, Melody T, Daniels R, et al. The impact of compliance with 6-hour and 24-hour sepsis bundles on hospital mortality in patients with severe sepsis: a prospective observational study. Crit Care. 2005;9(6):R764-70.https://ccforum.biomedcentral.com/articles/10.1186/cc3909http://www.ncbi.nlm.nih.gov/pubmed/16356225?tool=bestpractice.com[33]Daniels R, Nutbeam I, McNamara G, et al. The sepsis six and the severe sepsis resuscitation bundle: a prospective observational cohort study. 2011 Jun;28(6):507-12.http://www.ncbi.nlm.nih.gov/pubmed/21036796?tool=bestpractice.com 脓毒症是一个疾病谱系,为宿主对感染的全身性应答失调。[34]Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016 Feb 23;315(8):801-10.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4968574/http://www.ncbi.nlm.nih.gov/pubmed/26903338?tool=bestpractice.com 有关脓毒症的诊断和治疗的详细信息,请参阅“成人及儿童脓毒症”这一主题。
急性肺栓塞
重度肺栓塞 (PE) 表现为突发呼吸困难、胸痛,并伴心动过速、呼吸急促、低血压、低氧血症和颈静脉怒张。来源于下肢深静脉系统和盆腔静脉的血栓是最常见的病因。其他内源性或外源性物质,例如脂肪、空气、羊水、肿瘤、椎体成形术粘连剂、硅胶、下腔静脉过滤器或心脏植入装置等,也可引起 PE,但相对少见。[35]Habek D, Habek JC. Nonhemorrhagic primary obstetric shock. Fetal Diagn Ther. 2008;23(2):140-5.http://www.ncbi.nlm.nih.gov/pubmed/18046073?tool=bestpractice.com[36]Wessman DE, Kim TT, Parrish JS. Acute respiratory distress following liposuction. Mil Med. 2007 Jun;172(6):666-8.http://www.ncbi.nlm.nih.gov/pubmed/17615855?tool=bestpractice.com[37]Cunliffe CH, Denton JS. A fatal complication of a vena caval filter associated with pulmonary thromboembolism. Am J Forensic Med Pathol. 2008 Jun;29(2):173-6.http://www.ncbi.nlm.nih.gov/pubmed/18520489?tool=bestpractice.com[38]Kim YJ, Lee JW, Park KW, et al. Pulmonary cement embolism after percutaneous vertebroplasty in osteoporotic vertebral compression fractures: incidence, characteristics, and risk factors. Radiology. 2009 Apr;251(1):250-9.http://www.ncbi.nlm.nih.gov/pubmed/19332856?tool=bestpractice.com
既往静脉性血栓栓塞病史、抗凝不足、制动、长期住院、旅行、血管通路及下肢损伤可能使患者容易发生肺栓塞。
酶联免疫吸附实验(ELISA)检测D-二聚体的阴性预测值、下肢多普勒超声检查呈阴性结果,以及肺通气灌注扫描呈现正常或接近正常结果的可能性相似。[39]Stein PD, Hull RD, Patel KC, et al. D-dimer for the exclusion of acute venous thrombosis and pulmonary embolism: a systematic review. Ann Intern Med. 2004 Apr 20;140(8):589-602.http://www.ncbi.nlm.nih.gov/pubmed/15096330?tool=bestpractice.com 胸部计算机断层扫描 (CT) 血管造影是诊断和排除 PE 的最佳研究方法。在接受诊断性评估以等待确诊肺栓塞的患者中,应立即给予支持治疗和经验抗凝(除非有禁忌),不得延迟。[40]Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016 Feb;149(2):315-52.http://www.ncbi.nlm.nih.gov/pubmed/26867832?tool=bestpractice.com
气胸
突发呼吸困难伴单侧胸痛可能提示急性气胸。自发性气胸可见于继发于胸膜下肺大泡的高瘦体型者或者吸食可卡因者。也可见于 HIV 感染患者。继发性气胸常见于有基础肺部疾病者,例如COPD、淋巴管平滑肌瘤病。
发生张力性气胸时,空气进入胸膜腔,压缩肺组织,并使纵隔向健侧移位。 使得心脏、肺脏功能衰竭,需要紧急救治。 查体可见患侧呼吸音消失,叩诊呈鼓音。 气管向健侧偏移。
张力性气胸是一种紧急情况。治疗方法包括立即使用大口径穿刺针在患侧锁骨中线第二肋间胸腔行穿刺减压。这种减压方法可作为管状胸廓造口术的过渡操作。张力性气胸的进展十分危急,没有时间行其他检查,而非张力性气胸的胸部 X 线检查提示部分或全部肺组织塌陷,单侧肺透光度增加。[41]Tschopp JM, Bintcliffe O, Astoul P, et al. ERS task force statement: diagnosis and treatment of primary spontaneous pneumothorax. Eur Respir J. 2015 Aug;46(2):321-35.http://erj.ersjournals.com/content/46/2/321.longhttp://www.ncbi.nlm.nih.gov/pubmed/26113675?tool=bestpractice.com
 张力性气胸空针减压 (needle decompression) 动画演示
张力性气胸空针减压 (needle decompression) 动画演示
急性瓣膜关闭不全
急性心脏瓣膜闭锁不全常由于急性心肌梗死后二尖瓣缺血改变引起乳头肌或腱索断裂所致, 少见原因为心内膜炎所致的瓣叶断裂。[44]Karabinos I, Papadopoulos A, Toutouzas P. Severe mitral regurgitation due to perforation of the mitral anterior leaflet. Eur J Echocardiogr. 2008 Jan;9(1):103-4.http://www.ncbi.nlm.nih.gov/pubmed/17602878?tool=bestpractice.com
出现急性呼吸困难的症状,及伴随收缩期杂音、低血压急性心力衰竭、心动过速和肺部啰音等体征。 虽通过临床表现可疑诊为急性瓣膜关闭不全,但确诊有赖于超声心动图。
虽然患者已使用血管扩张剂稳定了病情(有时还联用加压药、正性肌力药物和输液),仍有必要进行紧急心血管手术会诊。在患者等待手术治疗期间,可能不得不采用临时的机械循环辅助装置或主动脉内球囊反搏装置。[45]Baumgartner H, Falk V, Bax JJ, et al; ESC Scientific Document Group. 2017 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. 2017 Sep 21;38(36):2739-91.https://academic.oup.com/eurheartj/article-lookup/doi/10.1093/eurheartj/ehx391http://www.ncbi.nlm.nih.gov/pubmed/28886619?tool=bestpractice.com 即使应用这些措施,急性瓣膜闭锁不全患者的预期死亡率仍然较高。
充血性心力衰竭急性加重
心源性肺水肿是由于左心室舒张末期压力增加所致,表现为劳力性呼吸困难、端坐呼吸、夜间阵发性呼吸困难、颈静脉怒张、外周液体潴留,心脏听诊可闻及第三心音奔马律,肺部充血(肺部听诊可闻细小湿啰音)。患者可有心力衰竭病史。
典型的胸部 X 线特征包括肺静脉淤血的特征性体征,可能伴有心脏扩大。 [Figure caption and citation for the preceding image starts]: 急性肺水肿的胸部 X 线征象:肺泡影增多、水平裂积液、肋膈角圆钝。由SyedW.Yusuf,MBBS,MRCPI,和DanielLenihan,MD提供 [Citation ends].
[Figure caption and citation for the preceding image starts]: 急性肺水肿的胸部 X 线征象:肺泡影增多、水平裂积液、肋膈角圆钝。由SyedW.Yusuf,MBBS,MRCPI,和DanielLenihan,MD提供 [Citation ends].
超声心动图提示心房颤动,心脏收缩及舒张功能减退。 在合适的临床环境中,床旁超声检查显示 B 线,强烈提示急性肺水肿。[46]Wimalasena Y, Kocierz L, Strong D, et al. Lung ultrasound: a useful tool in the assessment of the dyspnoeic patient in the emergency department. Fact or fiction? Emerg Med J. 2018 Apr;35(4):258-66.http://www.ncbi.nlm.nih.gov/pubmed/28258097?tool=bestpractice.com [Figure caption and citation for the preceding image starts]: 单肋间隙的肺超声扫描显示 B 线(白色垂线)——曲型线列Wimalasena Y, Kocierz L, Strong D, et al.肺部超声:一种用于评估急诊科呼吸困难患者的有效手段。Fact or fiction?Emerg Med J. 2017 Mar 3. pii. [Citation ends].
[Figure caption and citation for the preceding image starts]: 单肋间隙的肺超声扫描显示 B 线(白色垂线)——曲型线列Wimalasena Y, Kocierz L, Strong D, et al.肺部超声:一种用于评估急诊科呼吸困难患者的有效手段。Fact or fiction?Emerg Med J. 2017 Mar 3. pii. [Citation ends].
低脑利钠肽(BNP)水平(<100ng/L[<100 pg/mL])或者低N末端B型脑钠钛前体(NT-proBNP)水平 有助于排除充血性心力衰竭。[47]Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017 Aug 8;136(6):e137-61.http://circ.ahajournals.org/content/136/6/e137.longhttp://www.ncbi.nlm.nih.gov/pubmed/28455343?tool=bestpractice.com[48]National Institute for Health and Care Excellence. Acute heart failure: diagnosis and management. October 2014 [internet publication].https://www.nice.org.uk/guidance/cg187
根据充血性心力衰竭的具体病因,可联用利尿剂、硝酸盐(以降低心脏前后负荷)、ACEI 和无创机械通气。
主动脉夹层
主动脉夹层更常影响中年和老年男性、已患心脏瓣膜病患者(例如双叶瓣主动脉瓣或主动脉缩窄),以及胶原病患者(例如马方综合征或 Ehlers-Danlos 综合征)。通常表现为呼吸困难、剧烈胸痛,可能放射至背部。且可能伴有低血压。周围血管系统的检查可能显示没有外周脉搏,或者上下肢测得的血压不同。
当胸部 X 线检查提示纵隔增宽时应怀疑升主动脉夹层,不过这一表现仅出现于约 50% 的患者中。[49]Holloway BJ, Rosewarne D, Jones RG. Imaging of thoracic aortic disease. Br J Radiol. 2011 Dec;84 Spec No 3:S338-54.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3473913/http://www.ncbi.nlm.nih.gov/pubmed/22723539?tool=bestpractice.com 采用急诊超声心动图或胸部 CT 血管造影进行确诊。 [Figure caption and citation for the preceding image starts]: 一名 71 岁男性的 CT 显示升主动脉 II 型夹层动脉瘤。 升主动脉近段周围的血肿(图 A-D)压迫右肺动脉,几乎阻断其通畅且限制了对应肺的灌注。Stougiannos PN,Mytas DZ,Pyrgakis VN。 主动脉夹层的切面变化:类肺栓塞的不寻常表征。 BMJ Case Reports 2009;doi:10.1136/bcr.2006.104414 [Citation ends].
[Figure caption and citation for the preceding image starts]: 一名 71 岁男性的 CT 显示升主动脉 II 型夹层动脉瘤。 升主动脉近段周围的血肿(图 A-D)压迫右肺动脉,几乎阻断其通畅且限制了对应肺的灌注。Stougiannos PN,Mytas DZ,Pyrgakis VN。 主动脉夹层的切面变化:类肺栓塞的不寻常表征。 BMJ Case Reports 2009;doi:10.1136/bcr.2006.104414 [Citation ends].
主动脉夹层的治疗由夹层部位而定。如果是 A 型(升主动脉)夹层导致出现外科急症,则最先进行内科治疗的是 B 型(降主动脉)夹层。B 型夹层的手术干预可用于治疗内科处理无效的患者。在 B 型夹层的初始治疗中,使用血管内治疗越来越普遍。[50]European Society of Cardiology. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases. 2015 [internet publication].https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Aortic-Diseases
心包填塞
急性心包填塞可能由急性心肌梗死所致左心室壁破裂、冠状动脉破裂、主动脉夹层和起搏器导线受损引起。 表现为呼吸困难、颈静脉和面部充血、休克、周围性紫绀和心动过速。
诊断主要通过胸部 X 线片提示心脏轮廓增大和心电图提示低电压,确诊依赖超声心动图。治疗包括紧急心包穿刺术和/或手术干预治疗。 [Figure caption and citation for the preceding image starts]: 心包填塞:入院胸部 X 线检查Usalan C, Atalar E, Vural FK. Pericardial tamponade in a 65-year-old woman. Postgrad Med J. 1999;75:183-184; 经允许使用。 [Citation ends].
[Figure caption and citation for the preceding image starts]: 心包填塞:入院胸部 X 线检查Usalan C, Atalar E, Vural FK. Pericardial tamponade in a 65-year-old woman. Postgrad Med J. 1999;75:183-184; 经允许使用。 [Citation ends].
肺挫伤
肺挫伤和血胸可能主要由钝器伤(例如机动车事故、坠落)或穿通伤(例如刺伤、枪伤)所致。在肺挫伤时,向内破裂或惯性力撕裂肺泡组织,造成肺部出血、肺水肿以及胸部 X 线和 CT 上显示片状或多处融合的浸润影。治疗主要包括支持治疗,且需要充分监测、供氧和肺部清创。[51]Ullman EA, Donley LP, Brady WJ. Pulmonary trauma emergency department evaluation and management. Emerg Med Clin North Am. 2003 May;21(2):291-313.http://www.ncbi.nlm.nih.gov/pubmed/12793615?tool=bestpractice.com
由于血液可能大量积聚于胸膜腔内,患者可能出现呼吸困难、循环衰竭和休克等血胸的表现。通过胸部 X 线诊断,采集胸腔积液样本进行确诊。治疗包括使用大口径胸腔导管引流胸腔积液并减少胸腔积液量。可能需要胸部手术评估以进行持续积液引流。
缓慢性心律失常
重度缓慢性心律失常包括完全性心脏传导阻滞伴缓慢逸博心律,可能表现为呼吸困难伴无力、头晕或晕厥。进行心电图诊断后,排除可逆原因(例如急性前壁或下壁心肌梗死、药物治疗、电解质紊乱、甲状腺功能减退或肾上腺机能不全)并植入起搏器。 [Figure caption and citation for the preceding image starts]: 心电图示完全性房室传导阻滞Brian Olshansky, MD, FAHA, FACC{0}收集,允许引用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 心电图示完全性房室传导阻滞Brian Olshansky, MD, FAHA, FACC{0}收集,允许引用 [Citation ends].
