口腔段吞咽困难,其病理学涉及舌头、口腔底、腭、扁桃体或可导致吞咽困难的其他口腔结构。在这种情况下该问题经常被视为吞咽起始困难。当舌根、咽喉肌或环咽的肌肉发生功能障碍时,咽部疾病可引起吞咽困难。这时最明显的主诉是感觉食物粘在咽喉部、吸入性肺炎、声嘶、咳嗽、喉咙疼痛,甚至出现耳部牵涉痛。食管处吞咽困难可能是由于食管运动障碍、内源性或外源性肿物、食管璞、食管环、反流疾病或食管下括约肌疾病。这些疾病很可能表现为食物在食管下段、颈部或胸部引起哽咽感、食物反流、胸痛、或烧心。事实上,吞咽困难是多因素的。例如,一位有颈椎骨赘及食管反流的老年患者可能咽部肌肉组织力量薄弱。每个问题本身可能并无大碍,但若合并则可能会造成严重的吞咽困难。
口咽部感染/炎症
感染(例如咽炎、食管念珠菌病、会厌炎和咽后脓肿)可引起吞咽困难,放疗和/或化疗引起的口腔黏膜炎也可引起吞咽困难。[7]Hutcheson KA, Lewin JS. Functional outcomes after chemoradiotherapy of laryngeal and pharyngeal cancers. Curr Oncol Rep. 2012 Apr;14(2):158-65.http://www.ncbi.nlm.nih.gov/pubmed/22249533?tool=bestpractice.com
口腔结构异常
扁桃体肥大
扁桃体肥大可以影响固体食物从口腔到咽部而导致吞咽困难。
可能与阻塞性睡眠呼吸暂停综合征、反复感染、打鼾有关。
舌扁桃体(位于舌根部)可能很难看到,但可能变得肥厚而妨碍吞咽。通过可曲性鼻咽镜检查或间接喉镜检查配合口腔镜来进行观察。 [Figure caption and citation for the preceding image starts]: 扁桃体肥大引起严重咽喉部狭窄来自 DrS. Charous 的收集 [Citation ends].
[Figure caption and citation for the preceding image starts]: 扁桃体肥大引起严重咽喉部狭窄来自 DrS. Charous 的收集 [Citation ends]. [Figure caption and citation for the preceding image starts]: 扁桃体肥大来自 DrS. Charous 的收集 [Citation ends].
[Figure caption and citation for the preceding image starts]: 扁桃体肥大来自 DrS. Charous 的收集 [Citation ends]. [Figure caption and citation for the preceding image starts]: 扁桃体肥大来自 DrS. Charous 的收集 [Citation ends].
[Figure caption and citation for the preceding image starts]: 扁桃体肥大来自 DrS. Charous 的收集 [Citation ends].
口腔肿瘤(尤其癌症)
可累及口腔内任何结构,长到足够大时,可引起梗阻,并妨碍食物运送。
通过侵犯周围组织结构,可影响任何结构的功能:例如,舌癌侵及口腔底部导致舌头运动受损,引起吞咽困难。
在吸烟和饮酒人群中更常见。
人乳头状瘤病毒 (HPV) 感染引起的累及舌根和扁桃体的鳞状细胞癌在不吸烟人群中越来越常见。
经常与疼痛、言语改变、颈部肿块或血痰有关。
牙列
口咽结构异常
食管憩室
位于食管上括约肌的近端
随着年龄增加,发病率增加;女性患者中较常见。
在 60 多岁和 70 多岁的人群中,患病率为 50%
与未完全消化食物的反流、间断性固体食物吞咽困难、口臭和唾液过度分泌有关。
钡餐是最好的诊断检查方法。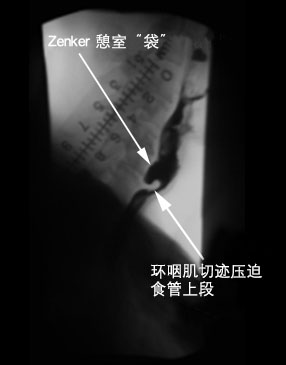 [Figure caption and citation for the preceding image starts]: 咽食管憩室(Zenker 憩室):吞钡食管 X 线检查的侧位片来自 DrS. Charous 的收集 [Citation ends].
[Figure caption and citation for the preceding image starts]: 咽食管憩室(Zenker 憩室):吞钡食管 X 线检查的侧位片来自 DrS. Charous 的收集 [Citation ends].
经食管内窥镜检查可漏诊或很难发现。[8]Cassivi SD, Deschamps C, Nichols FC, et al. Diverticula of the esophagus. Surg Clin North Am. 2005 Jun;85(3):495-503, ix.http://www.ncbi.nlm.nih.gov/pubmed/15927646?tool=bestpractice.com
咽/喉肿瘤
症状可能包括进行性固体食物吞咽困难、体重减轻、耳痛(牵涉性疼痛)。
嘶哑、误吸的症状(尤其是液体的)、呼吸短促经常与咽部肿瘤有关。
绝大多数恶性肿瘤是鳞状细胞癌,当这为原发部位时,经常具有很强的侵袭性,可出现频繁转移。
内窥镜检查和活检是最佳的诊断性试验。[9]Cook IJ, Kahrilas PJ. AGA technical review on the management of oropharyngeal dysphagia. Gastroenterology. 1999 Feb;116(2):455-78.http://www.ncbi.nlm.nih.gov/pubmed/9922328?tool=bestpractice.com [Figure caption and citation for the preceding image starts]: 喉/咽鳞状细胞癌来自 DrS. Charous 的收集 [Citation ends].
[Figure caption and citation for the preceding image starts]: 喉/咽鳞状细胞癌来自 DrS. Charous 的收集 [Citation ends].
狭窄
外源性压迫
颈部淋巴结肿大、环咽嵴、颈椎骨赘或甲状腺肿大。 [Figure caption and citation for the preceding image starts]: 咽的内镜视图显示骨赘向内压迫咽后壁,使背景中的喉和会厌无法看清来自 DrS. Charous 的收集 [Citation ends].
[Figure caption and citation for the preceding image starts]: 咽的内镜视图显示骨赘向内压迫咽后壁,使背景中的喉和会厌无法看清来自 DrS. Charous 的收集 [Citation ends]. [Figure caption and citation for the preceding image starts]: 吞钡时的侧位 X 线片显示骨赘使上段食管的钡剂流移位来自 DrS. Charous 的收集 [Citation ends].
[Figure caption and citation for the preceding image starts]: 吞钡时的侧位 X 线片显示骨赘使上段食管的钡剂流移位来自 DrS. Charous 的收集 [Citation ends]. [Figure caption and citation for the preceding image starts]: 甲状腺肿瘤压迫食管颈段来自 DrS. Charous 的收集 [Citation ends].
[Figure caption and citation for the preceding image starts]: 甲状腺肿瘤压迫食管颈段来自 DrS. Charous 的收集 [Citation ends].
可曲性光纤鼻咽镜检查/喉镜检查以及吞钡造影有助于确定是否有缺陷。
口咽神经肌肉异常
涉及中枢神经系统和运动神经元病或周围神经系统的神经肌肉失调可导致口腔和咽部吞咽困难。[10]Rothstein RD. A systematic approach to a patient with dysphagia. Hosp Pract (Minneap). 1997 Mar 15;32(3):169-75.http://www.ncbi.nlm.nih.gov/pubmed/9078978?tool=bestpractice.com 神经系统检查和神经症状评估有助于医生找到功能障碍的潜在的病因。以下是常见会导致口腔或咽部吞咽困难的神经肌肉疾病;卒中是最常见的原因:
卒中:约 40%-70% 的卒中患者有吞咽困难的经历[2]World Gastroenterology Organisation. WGO practice guideline - dysphagia. September 2014 [internet publication].http://www.worldgastroenterology.org/guidelines/global-guidelines/dysphagia
帕金森病[11]Sapir S, Ramig L, Fox C. Speech and swallowing disorders in Parkinson disease. Curr Opin Otolaryngol Head Neck Surg. 2008 Jun;16(3):205-10.http://www.ncbi.nlm.nih.gov/pubmed/18475072?tool=bestpractice.com[12]Potulska A, Friedman A, Królicki L, et al. Swallowing disorders in Parkinson's disease. Parkinsonism Relat Disord. 2003 Aug;9(6):349-53.http://www.ncbi.nlm.nih.gov/pubmed/12853234?tool=bestpractice.com
声带麻痹
肌萎缩侧索硬化
多发性硬化
大脑和颅底肿瘤
颅底切除或脑部肿瘤术后(尤其且经常涉及 IX、X、XII 颅神经)
干燥综合征[13]Mandl T, Ekberg O, Wollmer P, et al. Dysphagia and dysmotility of the pharynx and oesophagus in patients with primary Sjögren’s syndrome. Scand J Rheumatol. 2007 Sep-Oct;36(5):394-401.http://www.ncbi.nlm.nih.gov/pubmed/17963171?tool=bestpractice.com
重症肌无力
炎症性肌病
Wilson 病(肝豆状核变性)
进行性核上性麻痹
眼咽肌营养不良
肌肉紧张型吞咽困难,这是描述喉部和咽部过度紧张影响吞咽的新问题;它是言语治疗师做出的一种排除性诊断,还不能通过常规检查确诊。[14]Kang CH, Hentz JG, Lott DG. Muscle tension dysphagia: symptomology and theoretical framework. Otolaryngol Head Neck Surg. 2016 Nov;155(5):837-42.http://www.ncbi.nlm.nih.gov/pubmed/27352887?tool=bestpractice.com
食管结构异常
狭窄
主要症状是进食固体食物困难
胃镜或上消化道造影是最好的诊断检查方法。
当管腔直径<15 mm(正常为 20 mm)时,吞咽困难最为多见。[15]Schatzki R. The lower esophageal ring: long term follow-up of symptomatic and asymptomatic rings. Am J Roentegenol Radiat Ther Nucl Med. 1963 Oct;90:805-10.http://www.ncbi.nlm.nih.gov/pubmed/14068418?tool=bestpractice.com
酸反流占狭窄病例的 60%-70%,主要发生在食管下括约肌的区域。[16]Palmer ED. The hiatus hernia-esophagitis-esophageal stricture complex: twenty year prospective study. Am J Med. 1968 Apr;44(4):566-79.http://www.ncbi.nlm.nih.gov/pubmed/4868278?tool=bestpractice.com
腐蚀性药剂和放射治疗可能会导致食管狭窄。
氯化钾、多西环素、奎尼丁、非甾体抗炎药、铁和阿仑膦酸等药片可能引起狭窄。[17]Kikendall JW. Pill-induced esophageal injury. Gastroenterol Clin North Am. 1991 Dec;20(4):835-46.http://www.ncbi.nlm.nih.gov/pubmed/1787016?tool=bestpractice.com
食管壁内的病变
异物:急性吞咽困难可能由于异物和/或食物嵌塞食管所致。这些最常引起食管上或下括约肌处发生梗阻。
食管/贲门癌:患者通常表现为快速进展的固体食物吞咽困难;75% 的患者报告体重减轻。两种主要的类型是腺癌(50% 的病例)和鳞状细胞癌。最常发生在远端食管。食管胃十二指肠镜检查和活检通常为诊断方法。
良性肿瘤:罕见;包括平滑肌瘤、颗粒细胞肿瘤、乳头状瘤。
转移:远处转移发生在肺、肝、骨和脑。鳞状细胞癌局部浸润性比腺癌强。
食管外的病变压迫食管
纵隔肿块
支气管肺癌
颈椎骨关节炎/颈椎骨赘[18]Carlson ML, Archibald DJ, Graner DE, et al. Surgical management of dysphagia and airway obstruction in patients with prominent ventral cervical osteophytes. Dysphagia. 2011 Mar;26(1):34-40.http://www.ncbi.nlm.nih.gov/pubmed/20099000?tool=bestpractice.com
患者除有新增的吞咽困难症状外,通常还有原发疾病相关症状。
最好通过钡餐检查进行诊断。[9]Cook IJ, Kahrilas PJ. AGA technical review on the management of oropharyngeal dysphagia. Gastroenterology. 1999 Feb;116(2):455-78.http://www.ncbi.nlm.nih.gov/pubmed/9922328?tool=bestpractice.com
食管环
主要表现为间断性固体食物吞咽困难;如果发现,可推定为症状的原因。
黏膜环(Schatzki 环):患病率为 0.2%-1.4%。通常位于胃食管连接处。
肌肉环:位于胃食管连接处近端 1.5 cm 处。一般无症状。[19]Tobin RW. Esophageal rings, webs, and diverticula. J Clin Gastroenterol. 1998 Dec;27(4):285-95.http://www.ncbi.nlm.nih.gov/pubmed/9855256?tool=bestpractice.com
解剖学异常
食管憩室:被称为牵拉性憩室,由牵拉食管壁导致。位于食管的中 1/3 处。食管钡餐造影剂检查是最有用的检查方法。
食管裂孔疝:通常无症状,与胃食管反流病有关,可引起出血和嵌顿。
食管蹼:在接受食管胃十二指肠镜检查且病因为良性的吞咽困难患者中,发病率为 5%-15%。[19]Tobin RW. Esophageal rings, webs, and diverticula. J Clin Gastroenterol. 1998 Dec;27(4):285-95.http://www.ncbi.nlm.nih.gov/pubmed/9855256?tool=bestpractice.com
食管动力异常
特发性贲门失弛缓症
食管动力障碍性疾病主要表现为食管下括约肌松弛功能障碍和食管蠕动的受损。
继进食固体食物困难后出现吞咽液体食物困难这一表现见于 82%-100% 的患者。
食管测压有助于识别失弛症的动力异常。[20]Farrokhi F, Vaezi MF. Idiopathic (primary) achalasia. Orphanet J Rare Dis. 2007 Sep 26;2:38.http://www.ojrd.com/content/2/1/38http://www.ncbi.nlm.nih.gov/pubmed/17894899?tool=bestpractice.com[21]Patti MG, Gorodner MV, Gulvani C, et al. Spectrum of esophageal motility disorders: implications for diagnosis and treatment. Arch Surg. 2005 May;140(5):442-8; discussion 448-9.http://www.ncbi.nlm.nih.gov/pubmed/15897439?tool=bestpractice.com[22]Lacy BE, Weiser K. Esophageal motility disorders: medical therapy. J Clin Gastroenterol. 2008 May-Jun;42(5):652-8.http://www.ncbi.nlm.nih.gov/pubmed/18364589?tool=bestpractice.com[23]Smout AJ. Advances in esophageal motor disorders. Curr Opin Gastroenterol. 2008 Jul;24(4):485-9.http://www.ncbi.nlm.nih.gov/pubmed/18622164?tool=bestpractice.com
硬皮病
弥漫性食管痉挛
主要表现为与进食有关的发作性胸痛。
更常见于摄入过热或过冷食物的情况下。
通过测压诊断,检查结果显示同步收缩。[21]Patti MG, Gorodner MV, Gulvani C, et al. Spectrum of esophageal motility disorders: implications for diagnosis and treatment. Arch Surg. 2005 May;140(5):442-8; discussion 448-9.http://www.ncbi.nlm.nih.gov/pubmed/15897439?tool=bestpractice.com[22]Lacy BE, Weiser K. Esophageal motility disorders: medical therapy. J Clin Gastroenterol. 2008 May-Jun;42(5):652-8.http://www.ncbi.nlm.nih.gov/pubmed/18364589?tool=bestpractice.com[23]Smout AJ. Advances in esophageal motor disorders. Curr Opin Gastroenterol. 2008 Jul;24(4):485-9.http://www.ncbi.nlm.nih.gov/pubmed/18622164?tool=bestpractice.com[25]Richter JE, Castell DO. Diffuse esophageal spasm: reappraisal. Ann Intern Med. 1984 Feb;100(2):242-5.http://www.ncbi.nlm.nih.gov/pubmed/6691670?tool=bestpractice.com
吞钡检查发现同步收缩引起的“螺旋形”食管体。[21]Patti MG, Gorodner MV, Gulvani C, et al. Spectrum of esophageal motility disorders: implications for diagnosis and treatment. Arch Surg. 2005 May;140(5):442-8; discussion 448-9.http://www.ncbi.nlm.nih.gov/pubmed/15897439?tool=bestpractice.com [Figure caption and citation for the preceding image starts]: 吞钡检查时可见由弥漫性食管痉挛引起的螺旋形食管来自 DrS. Charous 的收集 [Citation ends].
[Figure caption and citation for the preceding image starts]: 吞钡检查时可见由弥漫性食管痉挛引起的螺旋形食管来自 DrS. Charous 的收集 [Citation ends].
食管收缩不足
可通过食管 X 线片或测压诊断。[22]Lacy BE, Weiser K. Esophageal motility disorders: medical therapy. J Clin Gastroenterol. 2008 May-Jun;42(5):652-8.http://www.ncbi.nlm.nih.gov/pubmed/18364589?tool=bestpractice.com[23]Smout AJ. Advances in esophageal motor disorders. Curr Opin Gastroenterol. 2008 Jul;24(4):485-9.http://www.ncbi.nlm.nih.gov/pubmed/18622164?tool=bestpractice.com
胡桃夹食管
与胸痛有关。
蠕动正常伴食管远端平均振幅增加,并且下食管括约肌压力增高。
诊断需要进行测压检查。[21]Patti MG, Gorodner MV, Gulvani C, et al. Spectrum of esophageal motility disorders: implications for diagnosis and treatment. Arch Surg. 2005 May;140(5):442-8; discussion 448-9.http://www.ncbi.nlm.nih.gov/pubmed/15897439?tool=bestpractice.com[22]Lacy BE, Weiser K. Esophageal motility disorders: medical therapy. J Clin Gastroenterol. 2008 May-Jun;42(5):652-8.http://www.ncbi.nlm.nih.gov/pubmed/18364589?tool=bestpractice.com[23]Smout AJ. Advances in esophageal motor disorders. Curr Opin Gastroenterol. 2008 Jul;24(4):485-9.http://www.ncbi.nlm.nih.gov/pubmed/18622164?tool=bestpractice.com[26]Katz PO, Dalton CB, Richter JE, et al. Esophageal testing of patients with noncardiac chest pain and/or dysphagia: result of a three year experience with 1161 patients. Ann Intern Med. 1987 Apr;106(4):593-7.http://www.ncbi.nlm.nih.gov/pubmed/3826958?tool=bestpractice.com
嗜酸性粒细胞性食管炎
男性的发病率是女性的 3-4 倍。成人的发病率比儿童更高,白种人的发病率比其他族群高。[27]Chen JW, Kao JY. Eosinophilic esophagitis: update on management and controversies. BMJ. 2017 Nov 13;359:j4482.http://www.ncbi.nlm.nih.gov/pubmed/29133286?tool=bestpractice.com
患者可能出现吞咽困难、烧心、胸痛、急性食物嵌塞和/或与胃食管反流相符的其他相关症状。[27]Chen JW, Kao JY. Eosinophilic esophagitis: update on management and controversies. BMJ. 2017 Nov 13;359:j4482.http://www.ncbi.nlm.nih.gov/pubmed/29133286?tool=bestpractice.com
食管胃十二指肠镜检查显示多个食管环伴随黏膜下纤维化和重塑引起的食管腔缩窄和弹性减低。[27]Chen JW, Kao JY. Eosinophilic esophagitis: update on management and controversies. BMJ. 2017 Nov 13;359:j4482.http://www.ncbi.nlm.nih.gov/pubmed/29133286?tool=bestpractice.com
通过内镜下食道黏膜活检明确诊断。[28]Roman S, Savarino E, Savarino V, et al. Eosinophilic oesophagitis: from physiopathology to treatment. Dig Liver Dis. 2013 Nov;45(11):871-8.http://www.sciencedirect.com/science/article/pii/S159086581300090Xhttp://www.ncbi.nlm.nih.gov/pubmed/23545170?tool=bestpractice.com[29]Dellon ES, Gonsalves N, Hirano I, et al. ACG clinical guideline: evidenced based approach to the diagnosis and management of esophageal eosinophilia and eosinophilic esophagitis (EoE). Am J Gastroenterol. 2013 May;108(5):679-92.https://www.nature.com/articles/ajg201371http://www.ncbi.nlm.nih.gov/pubmed/23567357?tool=bestpractice.com
