胸痛患者可根据病因是外伤性还是非外伤性进行分诊。评估非外伤性胸痛需要通过规范的流程,即在确定其他各种因素导致的胸痛之前,首先应排除急性心肌缺血。务必检查患者是否仍然感到疼痛,如果否,要查明其最后一次疼痛发作的时间。[18]National Institute for Health and Care Excellence. Chest pain of recent onset: assessment and diagnosis. November 2016 [internet publication].https://www.nice.org.uk/guidance/cg95
病史
应确定胸痛的特点,这有助于鉴别心源性、呼吸性、肌肉骨骼性疾病及其他病因。疼痛的类型、严重程度、部位和持续时间,是否有放散痛,以及加重和缓解的因素都有助于确定诊断。单纯依赖临床表现不能确诊急性冠状动脉综合征 (ACS)。[33]American Heart Association. Acute coronary syndromes. Circulation. 2005;112:III-55-III-72.https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.105.166475[34]Swap CJ, Nagurney JT. Value and limitations of chest pain history in the evaluation of patients with suspected acute coronary syndromes. JAMA. 2005 Nov 23;294(20):2623-9.http://jamanetwork.com/journals/jama/fullarticle/201900http://www.ncbi.nlm.nih.gov/pubmed/16304077?tool=bestpractice.com[35]Carlton EW, Than M, Cullen L, et al. 'Chest pain typicality' in suspected acute coronary syndromes and the impact of clinical experience. Am J Med. 2015 Oct;128(10):1109-16.e2.http://www.amjmed.com/article/S0002-9343(15)00360-5/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/25912206?tool=bestpractice.com
某些胸痛特点可为确诊发病原因提供线索。
压迫性疼痛可能由于心脏缺血或食管痉挛所致。
疼痛持续超过 15 分钟且表现为钝痛、中心性、压迫性,是 ACS 的特征之一。
疼痛放散至颌部或上肢提示心脏原因。[36]Fanaroff AC, Rymer JA, Goldstein SA, et al. Does this patient with chest pain have acute coronary syndrome? The rational clinical examination systematic review. JAMA. 2015 Nov 10;314(18):1955-65.http://www.ncbi.nlm.nih.gov/pubmed/26547467?tool=bestpractice.com
先前稳定型心绞痛患者新发疼痛或变为惯常模式,包括在几乎没有或根本没有劳累的情况下频繁反复发作,或持续时间超过 15 分钟,提示可能存在 ACS。[18]National Institute for Health and Care Excellence. Chest pain of recent onset: assessment and diagnosis. November 2016 [internet publication].https://www.nice.org.uk/guidance/cg95
吸气时尖锐的胸膜痛可能源于胸膜或心包,提示肺炎、肺栓塞或心包炎。
突发的胸骨后撕裂样疼痛并放散至后背部是典型的主动脉夹层的表现。
诱发或减轻胸痛的因素有助于鉴别心源性疾病与胃肠道疾病(例如胃食管反流病 [GORD]、消化性溃疡、食管痉挛)。心源性胸痛更可能由运动或情绪诱发,通常是在休息或使用硝酸酯类药物后缓解。然而,对硝酸甘油的治疗反应不应用于作出诊断。[18]National Institute for Health and Care Excellence. Chest pain of recent onset: assessment and diagnosis. November 2016 [internet publication].https://www.nice.org.uk/guidance/cg95 疼痛由进食、躺倒、热饮或饮酒引起,且使用抗酸剂可缓解,提示由胃肠道疾病原因引起。胃灼热和反酸是 GORD 的典型症状。[37]Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2013 Mar;108(3):308-28; quiz 329.http://www.ncbi.nlm.nih.gov/pubmed/23419381?tool=bestpractice.com 腹部疾病(例如急性胆囊炎和胰腺炎)也可能导致胸部牵涉性疼痛。
伴随症状可能有助于缩小诊断范围。呼吸困难是心脏缺血、肺栓塞 (PE)、气胸或肺炎患者的相关症状。恶心、呕吐和出汗可见于 ACS 患者。
除了这些较为典型的特征外,还应注意,部分 ACS 患者可能会出现非典型症状。这种情况在女性、糖尿病患者以及 75 岁以上老人中更常见。[38]Brieger D, Eagle KA, Goodman SG, et al; GRACE Investigators. Acute coronary syndromes without chest pain, an underdiagnosed and undertreated high-risk group: insights from the Global Registry of Acute Coronary Events. Chest. 2004 Aug;126(2):461-9.http://www.ncbi.nlm.nih.gov/pubmed/15302732?tool=bestpractice.com[39]Rich MW. Epidemiology, clinical features, and prognosis of acute myocardial infarction in the elderly. Am J Geriatr Cardiol. 2006 Jan-Feb;15(1):7-11; quiz 12.http://www.ncbi.nlm.nih.gov/pubmed/16415640?tool=bestpractice.com[40]Bayer AJ, Chadha JS, Farag PR, et al. Changing presentation of myocardial infarction with increasing old age. J Am Geriatr Soc. 1986 Apr;34(4):263-6.http://www.ncbi.nlm.nih.gov/pubmed/3950299?tool=bestpractice.com[41]Jacoby RM, Nesto RW. Acute myocardial infarction in the diabetic patient: pathophysiology, clinical course and prognosis. J Am Coll Cardiol. 1992 Sep;20(3):736-44.http://www.onlinejacc.org/content/20/3/736http://www.ncbi.nlm.nih.gov/pubmed/1512357?tool=bestpractice.com[42]McSweeney JC, Cody M, O'Sullivan P, et al. Women's early warning symptoms of acute myocardial infarction. Circulation. 2003 Nov 25;108(21):2619-23.http://circ.ahajournals.org/content/108/21/2619.longhttp://www.ncbi.nlm.nih.gov/pubmed/14597589?tool=bestpractice.com[43]DeVon HA, Pettey CM, Vuckovic KM, et al. A review of the literature on cardiac symptoms in older and younger women. J Obstet Gynecol Neonatal Nurs. 2016 May-Jun;45(3):426-37.http://www.ncbi.nlm.nih.gov/pubmed/26968243?tool=bestpractice.com
既往病史和特异性心脏危险因素(例如已知的心脏疾病、胆固醇水平增高、高血压、吸烟和家族史)都提示心源性原因。[44]National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III): final report. Circulation. 2002 Dec 17;106(25):3143-421.http://circ.ahajournals.org/content/106/25/3143.shorthttp://www.ncbi.nlm.nih.gov/pubmed/12485966?tool=bestpractice.com 使用可卡因同样更加可能导致心脏缺血。[45]McCord J, Jneid H, Hollander JE, et al; American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology. Management of cocaine-associated chest pain and myocardial infarction: a scientific statement from the American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology. Circulation. 2008 Apr 8;117(14):1897-907.http://circ.ahajournals.org/content/117/14/1897.fullhttp://www.ncbi.nlm.nih.gov/pubmed/18347214?tool=bestpractice.com 确定患者既往是否接受过任何胸痛检查或治疗会有帮助。[18]National Institute for Health and Care Excellence. Chest pain of recent onset: assessment and diagnosis. November 2016 [internet publication].https://www.nice.org.uk/guidance/cg95
同时应收集详尽的用药史(例如应用非甾体抗炎药 [non-steroidal anti-inflammatory drugs, NSAID] 可能是胃病的病因)。
体格检查
体格检查可进一步缩小鉴别诊断的范围。
胸痛患者可能出现急性休克,如患有下列疾病的患者:
张力性气胸
心脏压塞
大面积肺栓塞
伴心源性休克的 ACS
胰腺炎
肺炎或胆囊炎导致的脓毒症
食管破裂。
心脏体格检查能够发现的异常情况包括脉搏或心音异常(例如新发的主动脉狭窄或现有杂音加重)、低血压或高血压以及心力衰竭体征。
听诊发现单侧或双侧肺底捻发音提示肺炎或心力衰竭。单侧呼吸音减低可由气胸或局灶性肺叶塌陷导致。
胸痛区域触诊有压痛通常提示肌肉骨骼疾病,例如肋软骨炎。然而,许多心肌梗死患者就诊时也有胸壁疼痛。沿皮区分布(有或没有典型皮疹)的单侧压痛可能提示带状疱疹。疼痛通常持续 2-3 天,随后受累皮区出现皮疹。不过,一些患者在出疹前会出现持续约 1 周的疼痛。[46]Dworkin RH, Johnson RW, Breuer J, et al. Recommendations for the management of herpes zoster. Clin Infect Dis. 2007 Jan 1;44 Suppl 1:S1-26.https://academic.oup.com/cid/article/44/Supplement_1/S1/334966/Recommendations-for-the-Management-of-Herpeshttp://www.ncbi.nlm.nih.gov/pubmed/17143845?tool=bestpractice.com 通常情况下,皮疹为具有红色基底部的水疱,分布于皮区的单侧。 [Figure caption and citation for the preceding image starts]: 水痘带状疱疹病毒由 Daniel Eisen, MD 提供;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 水痘带状疱疹病毒由 Daniel Eisen, MD 提供;经许可后使用 [Citation ends].
除非有持续存在但稳定的共病,否则胃肠道原因引起的胸痛通常与心脏和呼吸检查结果正常相关。腹部检查异常(压痛、反跳痛和腹肌紧张)使得胃肠道病因的可能性更大。可能的疾病包括:GORD、消化性溃疡 (peptic ulcer disease, PUD)、胆囊炎、胰腺炎和胃炎。
基础检查
基本检查指标包括体温、血压、脉搏和呼吸频率。此外,也应对以下指标进行监测,基于临床判断确定所需的监测频率,直至作出明确诊断。[18]National Institute for Health and Care Excellence. Chest pain of recent onset: assessment and diagnosis. November 2016 [internet publication].https://www.nice.org.uk/guidance/cg95
心律
脉搏血氧测量得出的血氧饱和度
重复静息态 12 导联心电图
任何疼痛和/或其他症状的加重
疼痛缓解;确认疼痛缓解有效。
心电图 (ECG)
多数患者需行 12 导联心电图 (ECG) 检查,除非能够确信是非心源性疾病(例如气胸)。应在患者就诊后尽快进行 ECG。在心脏原因中,ST 段改变(例如 ST 段抬高或 ST 段压低)、QRS 波群异常、心律失常或者心动过速或心动过缓均是特征性发现。
相邻导联的 ST 段抬高(在 J 点测量)>1 mm 提示 ST 段抬高型心肌梗死 (ST-elevation myocardial infarction, STEMI)。相邻导联 ST 段压低或 T 波倒置可能提示冠状动脉缺血。ACS 患者的可能有正常或近乎正常的 ECG;如果怀疑有 ACS,应进行连续 ECG 检查。 [Figure caption and citation for the preceding image starts]: 心电图显示急性下壁心肌梗死的改变,即 II、III 和 aVF 导联 ST 段抬高由 James Brown 教授提供;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 心电图显示急性下壁心肌梗死的改变,即 II、III 和 aVF 导联 ST 段抬高由 James Brown 教授提供;经许可后使用 [Citation ends].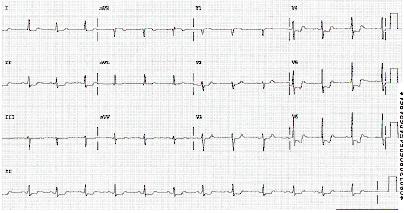 [Figure caption and citation for the preceding image starts]: 心电图显示 ST 段压低来自休斯顿德克萨斯大学心脏内科 Syed W. Yusuf 医生和 Iyad N. Daher 医生的个人收集;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 心电图显示 ST 段压低来自休斯顿德克萨斯大学心脏内科 Syed W. Yusuf 医生和 Iyad N. Daher 医生的个人收集;经许可后使用 [Citation ends].
心包炎可能表现为弥漫性 ST 段抬高伴 PR 段压低。
肺栓塞患者可能存在的心电图表现包括窦性心动过速(最常见)、I 导联 S 波伴 III 导联 Q 波和 T 波倒置(S I、Q III、T III 形态)。
心包填塞患者可能会出现心电交替。
胸部 X 线检查
胸部 X 线检查 (CXR ) 可证实一些呼吸系统疾病,例如气胸或肺炎。如果担心肺炎(并且患者的临床情况足够稳定,能转送到放射科),则后前位 (posterior-anterior, PA) 和侧位投影可增加诊断的敏感性。心脏缺血患者的胸部 X 线检查结果经常正常,但是该检查可为严重心脏病变提供线索,例如主动脉夹层时的纵隔增宽、心脏压塞时的巨大球形心脏。 [Figure caption and citation for the preceding image starts]: 胸部 X 线检查显示纵隔增宽由 James Brown 教授提供;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 胸部 X 线检查显示纵隔增宽由 James Brown 教授提供;经许可后使用 [Citation ends]. [Figure caption and citation for the preceding image starts]: 一名心包填塞患者的胸部 X 线检查显示大的球形心脏由 James Brown 教授提供;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 一名心包填塞患者的胸部 X 线检查显示大的球形心脏由 James Brown 教授提供;经许可后使用 [Citation ends].
血液检测
对于担心急性冠脉综合征的患者,就诊时应进行心脏生化标志物检查,并在就诊后每 6 至 8 小时复查一次。具体方案存在很大差异,这取决于现有的生物标志物类型。[21]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014 Dec 23;130(25):e344-426.http://circ.ahajournals.org/content/130/25/e344.longhttp://www.ncbi.nlm.nih.gov/pubmed/25249585?tool=bestpractice.com[47]Roffi M, Patrono C, Collet JP et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016 Jan 14;37(3):267-315.https://academic.oup.com/eurheartj/article/37/3/267/2466099/2015-ESC-Guidelines-for-the-management-of-acutehttp://www.ncbi.nlm.nih.gov/pubmed/26320110?tool=bestpractice.com
在多种情况下,包括心肌梗死、跌倒或癫痫发作后、肌炎、低体温或甲状腺功能减退等,见于骨骼肌和心肌的心脏生化标志物(例如肌钙蛋白 I 或 T、肌酸激酶 [reatine kinase, CK]、肌酸激酶同工酶 MB [creatine kinase-MB, CK-MB])升高。对于心肌损伤,肌钙蛋白比肌酸激酶 (CK) 或肌酸激酶同工酶 MB (CK-MB) 更具特异性。在评估胸痛患者时,肌钙蛋白是首选的生物标记物。如果高敏肌钙蛋白检测可用,则可以更早的诊断急性冠脉综合征。[48]Mueller C, Giannitsis E, Christ M, et al. Multicenter evaluation of a 0-hour/1-hour algorithm in the diagnosis of myocardial infarction with high-sensitivity cardiac troponin T. Ann Emerg Med. 2016 Jul;68(1):76-87.e4.http://www.annemergmed.com/article/S0196-0644(15)01501-2/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/26794254?tool=bestpractice.com 非缺血性心电图和高敏肌钙蛋白 T 阴性的患者,特别是如果患者疼痛超过 3 小时,其发生主要不良心脏事件 (major adverse cardiac events, MACE) 的风险非常低。[49]National Institute for Health and Care Excellence. Myocardial infarction (acute): early rule out using high-sensitivity troponin tests (Elecsys Troponin T high-sensitive, ARCHITECT STAT High Sensitive Troponin-I and AccuTnI+3 assays). October 2014 [internet publication].https://www.nice.org.uk/guidance/dg15/chapter/1-Recommendations[50]Pickering JW, Than MP, Cullen L, et al. Rapid rule-out of acute myocardial infarction with a single high-sensitivity cardiac troponin T measurement below the limit of detection: a collaborative meta-analysis. Ann Intern Med. 2017 May 16;166(10):715-24.http://eprints.whiterose.ac.uk/116205/1/Pickering%20Than%20MS%20AnnIntMed%20R1%20Clean%20Accepted.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/28418520?tool=bestpractice.com 在英国,英国国家卫生与临床优化研究所 (National Institute for Health and Care Excellence, NICE) 于 2016 年更新了关于胸痛评估的指南,对于不怀疑 ACS 的患者,不推荐进行高敏肌钙蛋白检测。[18]National Institute for Health and Care Excellence. Chest pain of recent onset: assessment and diagnosis. November 2016 [internet publication].https://www.nice.org.uk/guidance/cg95 一项针对伴胸痛但无 ACS 的急诊科患者的队列研究发现,在三年的平均随访时间内,任何高敏肌钙蛋白的升高都会增加心血管事件和死亡风险。 [51]Roos A, Bandstein N, Lundbäck M,et al. Stable high-sensitivity cardiac troponin T levels and outcomes in patients with chest pain. J Am Coll Cardiol. 2017 Oct 31;70(18):2226-36.http://www.onlinejacc.org/content/70/18/2226http://www.ncbi.nlm.nih.gov/pubmed/29073949?tool=bestpractice.com只有肌钙蛋白检测不可用时,才使用肌酸激酶检测。
应进行全血细胞计数 (full blood count, FBC),以筛查贫血和感染证据。
作为基线检查肾功能检查很有用。
在进行病史询问、体格检查和基本检查后,能排除或证实一些胸痛的鉴别诊断。这些鉴别诊断包括 ST 段抬高型心肌梗死 (ST-elevation myocardial infarction, STEMI)、气胸、肺炎、心包炎和肋软骨炎。第 2 组心脏生化标志物的结果通常能证实非 ST 段抬高型心肌梗死 (non-ST-elevation myocardial infarction, NSTEMI) 的诊断。如果患者的连续心电图检查结果正常,并且 2 组肌钙蛋白检测结果正常(间隔至少 3 小时),可考虑在接下来的 72 小时内进行门诊检查。[21]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014 Dec 23;130(25):e344-426.http://circ.ahajournals.org/content/130/25/e344.longhttp://www.ncbi.nlm.nih.gov/pubmed/25249585?tool=bestpractice.com
伴经皮冠状动脉介入治疗 (percutaneous coronary intervention, PCI) 的冠状动脉造影
对于存在诸如胸痛持续不缓解和心电图动态改变等高危特征的 STEMI 和 NSTEMI 患者,需要尽快行冠状动脉造影和 PCI。 [Figure caption and citation for the preceding image starts]: 血管造影显示右侧动脉闭塞来源于 Mahi Ashwath 医生的个人收集;获得允许后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 血管造影显示右侧动脉闭塞来源于 Mahi Ashwath 医生的个人收集;获得允许后使用 [Citation ends].
如果无 PCI 可用或需要延迟 2 小时以上才能进行,则对 STEMI 患者应进行全身性纤维蛋白溶解治疗,但这不适用于 NSTEMI。
风险分层
已经开发出 HEART 评分,用于急诊科患者的风险分层。HEART 评分低 (0-3) 的患者在 6 周时发生主要不良心脏事件 (major adverse cardiac event, MACE) 的风险较低。HEART 评分高 (7-10) 的患者发生 MACE 的风险很高。[36]Fanaroff AC, Rymer JA, Goldstein SA, et al. Does this patient with chest pain have acute coronary syndrome? The rational clinical examination systematic review. JAMA. 2015 Nov 10;314(18):1955-65.http://www.ncbi.nlm.nih.gov/pubmed/26547467?tool=bestpractice.com[52]Backus BE, Six AJ, Kelder JC, et al. A prospective validation of the HEART score for chest pain patients at the emergency department. Int J Cardiol. 2013 Oct 3;168(3):2153-8.http://www.internationaljournalofcardiology.com/article/S0167-5273(13)00315-X/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/23465250?tool=bestpractice.com[53]Poldervaart JM, Reitsma JB, Backus BE, et al. Effect of using the HEART score in patients with chest pain in the emergency department: a stepped-wedge, cluster randomized trial. Ann Intern Med. 2017 May 16;166(10):689-97.http://www.ncbi.nlm.nih.gov/pubmed/28437795?tool=bestpractice.com
 [Figure caption and citation for the preceding image starts]: 适用于急诊科胸痛患者的 HEART 评分构成Six AJ, et al. Neth Heart J. 2008;16:191-6; 经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 适用于急诊科胸痛患者的 HEART 评分构成Six AJ, et al. Neth Heart J. 2008;16:191-6; 经许可后使用 [Citation ends].
还有很多其他可用的风险评分。相关指南针对到急诊室就诊的急性胸痛患者的风险分层建议不尽相同。[54]American College of Cardiology. The use of chest pain scores and high-sensitivity troponin for evaluating chest pain patients. May 2016 [internet publication].http://www.acc.org/latest-in-cardiology/articles/2016/03/18/08/28/the-use-of-chest-pain-scores-and-high-sensitivity-troponin
进一步调查
一些患者需要进一步检查以确定疑似诊断。
一旦排除 ACS、室性心律失常和血流动力学不稳定,对于临床上考虑胸痛由缺血引发的患者,可以根据心绞痛的可能性和冠状动脉疾病 (CAD) 风险进行分层。[55]American College of Radiology. ACR appropriateness criteria: chest pain suggestive of acute coronary syndrome. 2014 [internet publication].https://acsearch.acr.org/docs/69403/Narrative/[56]Wolk MJ, Bailey SR, Doherty JU, et al; American College of Cardiology Foundation Appropriate Use Criteria Task Force. ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013 multimodality appropriate use criteria for the detection and risk assessment of stable ischemic heart disease. J Am Coll Cardiol. 2014 Feb 4;63(4):380-406.http://www.onlinejacc.org/content/63/4/380http://www.ncbi.nlm.nih.gov/pubmed/24355759?tool=bestpractice.com[57]Morise AP, Haddad WJ, Beckner D. Development and validation of a clinical score to estimate the probability of coronary artery disease in men and women presenting with suspected coronary disease. Am J Med. 1997 Apr;102(4):350-6.http://www.ncbi.nlm.nih.gov/pubmed/9217616?tool=bestpractice.com[58]Pryor DB, Shaw L, McCants CB, et al. Value of the history and physical in identifying patients at increased risk for coronary artery disease. Ann Intern Med. 1993 Jan 15;118(2):81-90.http://www.ncbi.nlm.nih.gov/pubmed/8416322?tool=bestpractice.com[59]Diamond GA, Forrester JS. Analysis of probability as an aid in the clinical diagnosis of coronary-artery disease. N Engl J Med. 1979 Jun 14;300(24):1350-8.http://www.ncbi.nlm.nih.gov/pubmed/440357?tool=bestpractice.com[60]Pryor DB, Harrell FE Jr., Lee KL, et al. Estimating the likelihood of significant coronary artery disease. Am J Med. 1983 Nov;75(5):771-80.http://www.ncbi.nlm.nih.gov/pubmed/6638047?tool=bestpractice.com
CAD 的验前概率较高 (>90%):应行冠状动脉造影。
CAD 的验前概率中等 (10-90%):应进行负荷试验及影像学检查(放射性核素、超声心动图或磁共振成像)。
CAD 的验前概率低 (<10%):如果可从患者心电图进行判读(不是左束支传导阻滞、预激 [Wolff-Parkinson-White] 或心室起搏节律)并且患者能够运动,则其应该进行运动负荷试验。否则,患者应该进行负荷试验及影像学检查。[55]American College of Radiology. ACR appropriateness criteria: chest pain suggestive of acute coronary syndrome. 2014 [internet publication].https://acsearch.acr.org/docs/69403/Narrative/
各相关指南针对使用风险分层和进一步具体检查的建议有所不同,因此查阅当地诊疗规范很重要。
对于无心绞痛症状的患者,应评估胸痛的其他原因。
经胸超声心动图是评价心脏功能的无创手段。如果疑似心脏填塞,实施超声心动图检查非常必要,它还有助于确诊肺动脉高压。
为了作出主动脉夹层的诊断,CT 血管造影更为有用。如果有擅长夹层诊断的操作者,则经食管超声心动图是一种替代方法。[61]American College of Radiology. ACR appropriateness criteria: acute chest pain - suspected aortic dissection. 2014 [internet publication].https://acsearch.acr.org/docs/69402/Narrative/
PE 可能难以诊断。需保持高度警觉。初始检查包括胸部 X 线检查、心电图和动脉血气分析 (arterial blood gases, ABG),但这些检查的结果并不能确定或排除 PE 的诊断。经过验证的评分有助于预测 PE 的可能性。其中包括 Wells 评分和 Geneva 评分(及其简化版本)。[62]Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients' probability of pulmonary embolism: increasing the model's utility with the SimpliRED D-dimer. Thromb Haemost. 2000 Mar;83(3):416-20.http://www.ncbi.nlm.nih.gov/pubmed/10744147?tool=bestpractice.com[63]Le Gal G, Righini M, Roy PM, et al. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med. 2006 Feb 7;144(3):165-71.http://www.ncbi.nlm.nih.gov/pubmed/16461960?tool=bestpractice.com 通过酶联免疫吸附法的 D-二聚体血液检验的敏感性和阴性预测值>95%(不考虑估算的临床可能性),可有效排除存在静脉血栓栓塞。不过,特异性要低得多,估计为 23%-63%。对于临床可能性评估为低或中等的患者,此种方法尤为有效。[64]Righini M, Perrier A, De Moerloose P, et al. D-dimer for venous thromboembolism diagnosis: 20 years later. J Thromb Haemost. 2008 Jul;6(7):1059-71.http://onlinelibrary.wiley.com/doi/10.1111/j.1538-7836.2008.02981.x/fullhttp://www.ncbi.nlm.nih.gov/pubmed/18419743?tool=bestpractice.com[65]Dunn KL, Wolf JP, Dorfman DM, et al. Normal D-dimer levels in emergency department patients suspected of acute pulmonary embolism. J Am Coll Cardiol. 2002 Oct 16;40(8):1475-8.http://www.onlinejacc.org/content/40/8/1475http://www.ncbi.nlm.nih.gov/pubmed/12392839?tool=bestpractice.com[66]Crawford F, Andras A, Welch K, Sheares K, Keeling D, Chappell FM. D-dimer test for excluding the diagnosis of pulmonary embolism. Cochrane Database Syst Rev. 2016 Aug 5;(8):CD010864.https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD010864.pub2/fullhttp://www.ncbi.nlm.nih.gov/pubmed/27494075?tool=bestpractice.com
对于确定为 PE 风险极低的患者,可使用肺栓塞排除标准 (Pulmonary Embolism Rule-Out Criteria, PERC)。如果患者符合所有标准(年龄<50 岁;初始心率<100 次/分;呼吸室内空气情况下初始氧饱和度>94%;无单侧腿部肿胀;无咯血;在最近 4 周内无手术或创伤;无静脉血栓栓塞病史;未使用雌激素),则认为 PE 的风险低于检测的风险,因此不需要行 D-二聚体检测。应对不符合所有标准的患者行 D-二聚体检测。[67]Raja AS, Greenberg JO, Qaseem A, et al. Evaluation of patients with suspected acute pulmonary embolism: best practice advice from the Clinical Guidelines Committee of the American College of Physicians. Ann Intern Med. 2015 Nov 3;163(9):701-11.http://annals.org/aim/article/2443959/evaluation-patients-suspected-acute-pulmonary-embolism-best-practice-advice-fromhttp://www.ncbi.nlm.nih.gov/pubmed/26414967?tool=bestpractice.com
对于依据临床评分判断为 PE 可能性较低且未见 D-二聚体水平升高的患者,可有效排除 PE 的诊断。这类患者在近 3 个月内发生 PE 的风险小于 1%。[68]Carrier M, Righini M, Djurabi RK, et al. VIDAS D-dimer in combination with clinical pre-test probability to rule out pulmonary embolism: a systematic review of management outcome studies. Thromb Haemost. 2009 May;101(5):886-92.http://www.ncbi.nlm.nih.gov/pubmed/19404542?tool=bestpractice.com
对于依据临床评分判断为 PE 可能性高(即可能为 PE)或存在 D-二聚体异常的患者,需要进行影像学检查。胸部多排计算机断层扫描肺动脉造影 (computed tomographic pulmonary angiography, CTPA) 是首选的影像学检查方法。 [Figure caption and citation for the preceding image starts]: 螺旋 CT 肺血管造影显示肺血管内有大型充盈缺损,与鞍状栓子相符由 James Brown 教授提供;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 螺旋 CT 肺血管造影显示肺血管内有大型充盈缺损,与鞍状栓子相符由 James Brown 教授提供;经许可后使用 [Citation ends].
如果有 CTPA 禁忌证或者不可用,可以采用其他影像学检查,例如肺通气/灌注扫描。
如果胸痛更可能是胃肠道原因,应考虑行食管胃十二指肠镜、食管 PH 值监测、食管测压、钡餐和幽门螺杆菌呼气试验检查。一旦排除胸痛的心源性病因,可以使用质子泵抑制剂试验性治疗,减轻 GORD 患者的症状。[69]Wang WH, Huang JQ, Zheng GF, et al. Is proton pump inhibitor testing an effective approach to diagnose gastroesophageal reflux disease in patients with noncardiac chest pain?: a meta-analysis. Arch Intern Med. 2005 Jun 13;165(11):1222-8.http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/486601http://www.ncbi.nlm.nih.gov/pubmed/15956000?tool=bestpractice.com
如疑诊急性胆囊炎或急性胰腺炎,则有必要进一步进行肝功能和血清脂肪酶等血液检查。 这些诊断可能还需进一步影像学检查,例如腹部超声检查和腹部 CT(用于急性胰腺炎)。
 张力性气胸空针减压 (needle decompression) 动画演示
张力性气胸空针减压 (needle decompression) 动画演示
 静脉穿刺和抽血的动画演示
静脉穿刺和抽血的动画演示
 关于如何进行心电图的动画演示
关于如何进行心电图的动画演示
