多种因素参与了心动过速的发生,其病因学并不确定。最常见类型是窦性心动过速。对于非窦率增加的快速性心律失常患者而言,其原因是组织内传导的异质性引起自律性增高、触发活动或折返从而导致组织局灶快速电活动。其次为包括离子通道病、心肌坏死疤痕、外科手术疤痕、心房或心室室壁张力增高和充盈压升高所致的牵张、缺血、离子紊乱、内源性儿茶酚胺增加、滥用药物、心肌炎或上述多种因素并存。
室率规则的窄QRS波群(<120ms)
窦性心动过速:起源于窦房结,心率每分钟100次以上。这常常是机体对于躯体、情感、心理变化或药物的正常反应。其次原因包括躯体去适应状态,组织缺氧,肺动脉栓塞,低容量血症,甲状腺机能亢进,贫血,药物(如咖啡因、酒精、尼古丁、安非他明、可卡因)和处方药物(氨茶碱、阿托品、儿茶酚胺等)。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com另一个考虑是体位性直立性心动过速综合征(POTS),特征为心室率过快(站立位或直立倾斜时10分钟内心率增加30次以上或绝对心率增加至120次以上),以及伴随直立位症状。 其前提是排除窦性心动过速的心脏原因。[9]Benarroch EE. Postural tachycardia syndrome: a heterogeneous and multifactorial disorder. Mayo Clin Proc. 2012;87:1214-1225.http://www.mayoclinicproceedings.org/article/S0025-6196%2812%2900896-8/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/23122672?tool=bestpractice.com处理方面主要是对因治疗,因此寻找诸如低血容量、低氧、甲状腺功能亢进、疼痛、焦虑、使用兴奋剂或药物等原因。
不适当窦性心动过速指静息时心率持续增快,与躯体、情感、病理变化或药物使用无关或不成比例(静息心率>100次/分或24小时动态心电图监测平均心率>90次/分)。确切病因不明,很可能是多因素参与。可能原因还有窦房结自律性增高和自主神经机能障碍。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com
房性心动过速:快速心房活动来源于心房一个区域而非窦房结,心率在100-250次/分。多源性房性心动过速指心房活动有3个或以上心房激活灶(一般不规则)。局灶房性心动过速可见于无心脏病者。伴房室组织的房性心动过速应警惕洋地黄中毒。低钾血症也能加重这种状态。[10]Steinbeck G, Hoffmann E. 'True' atrial tachycardia. Eur Heart J. 1998;19(Suppl E):E10-E12,E48-E49.http://www.ncbi.nlm.nih.gov/pubmed/9717019?tool=bestpractice.com右侧房性心动过速起源于界嵴、三尖瓣环或冠状窦口。左侧房性心动过速常起源于肺静脉周围、房间隔或二尖瓣环。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com
心房扑动: [Figure caption and citation for the preceding image starts]: 心房扑动资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 心房扑动资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].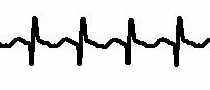 [Figure caption and citation for the preceding image starts]: 心房扑动(详细内容)资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].房扑是心房大区域的折返活动节律,心房率在250-350次/分,心室率常在145-150次/分(2:1阻滞)。经典房扑是心房巨大折返环沿三尖瓣或下腔静脉与三尖瓣环之间转动。射频消融靶标本质即是针对这一折返环。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: 心房扑动(详细内容)资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].房扑是心房大区域的折返活动节律,心房率在250-350次/分,心室率常在145-150次/分(2:1阻滞)。经典房扑是心房巨大折返环沿三尖瓣或下腔静脉与三尖瓣环之间转动。射频消融靶标本质即是针对这一折返环。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com
窦房结折返性心动过速:起源于窦房结和结旁组织的折返环,据认为是基于窦房结和窦旁组织的异质性传导特性。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com
房室结折返性心动过速(AVNRT):折返性心动过速涉及房室结内或结旁心房组织两条旁道。一条旁道是快传导径路,不应期相对较长;一条旁道属于慢传导径路,不应期较短。早发房性冲动之后,快径路仍处于先前冲动的不应期内,从而通过慢径路(脱离不应期)进行前向传导。当慢径路传导结束时,快径路已经脱离不应期,则可发生逆向传导。如果慢径路在逆向传导后脱离不应期,折返会反复出现。AVNRT(非典型AVNRT)少见一个类型涉及前向传导至快径路,形成与前已描述常见经典AVNRT反向的折返环路。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com
房室折返性心动过速(AVRT):折返性心动过速环路涉及一条辅助旁路和房室结本身。最常见类型(超过95%)是顺向性房室折返心动过速。心律不齐由经由房室 (AV) 结的前向传导和经由附加旁路的逆行传导所致。由于通过希氏-浦肯野系统激动心室,所以形成窄QRS波心动过速。[11]Gillette PC, Garson AJ, Kugler JD. Wolff-Parkinson-White syndrome in children: electrophysiologic and pharmacologic characteristics. Circulation. 1979;60:1487-1495.http://circ.ahajournals.org/cgi/reprint/60/7/1487http://www.ncbi.nlm.nih.gov/pubmed/498476?tool=bestpractice.com
持续性交界区反复性心动过速:属于顺向性AVRT的一种类型,通过房室结前向传导,经由附加旁路逆向传导。折返环逆向支的特点是慢传导,这导致折返环稳定(沿房室结前向传导,经慢传导旁道逆向回返)。术语“持续性”反映其稳定性和易于反复发作,成为主导心律。鉴于此,该心律失常有时引起心动过速性心肌病,心室率处在120-200次/分。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com最常见于婴儿和儿童。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com
交界区异位性心动过速:源自交界区(房室结远端或希氏-浦肯野系统近端)异常快速冲动释放,起源并未涉及心房或心室。先天类型较为隐匿,常在婴儿时做出诊断,这也仅见于发展成心动过速性心肌病之后才得以诊断。有时见于心脏外科手术后,由于室率快并且房室不同步而导致血流动力学不稳定。易患临床因素包括洋地黄中毒、低钾血症、心肌缺血、心脏外科手术和感染性心肌炎。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com
窄QRS群(<120ms)伴不规则心室率
心房颤动:属于室上性心动过速。 由于不规则冲动快速和随机性传导至心室,引起心室率绝对不等。不规则冲动是源于多折返波在心房内随机性转动,并随机性冲击房室结。[12]Fuster V, Ryden L, Cannom D, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation - executive summary. J Am Coll Cardiol. 2006;48:854-906.http://content.onlinejacc.org/article.aspx?articleid=1137853http://www.ncbi.nlm.nih.gov/pubmed/16904574?tool=bestpractice.com
伴房室传导多变的房性心动过速或房扑:与房颤相反,快速房性心动过速和房扑可造成抵达房室结的冲动快速而规则。下传至心室的冲动多变,但倾向呈现不规则中的规律性模式。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com
多源性房性心动过速:至少存在3个不同的完整心房灶,最常见于肺动脉疾病,也见于心脏病(心瓣膜病、高血压病和冠状动脉病变)和其他各系统疾病。包括低钾血症、低镁血症、脓毒血症和特定药物(异丙肾上腺素和氨茶碱)。[13]Shine KI, Kastor JA, Yurchak PM. Multifocal atrial tachycardia. Clinical and electrocardiographic features in 32 patients. N Engl J Med. 1968;279:344-349.http://www.ncbi.nlm.nih.gov/pubmed/5662166?tool=bestpractice.com[14]Iseri LT, Fairshter RD, Hardemann JL, et al. Magnesium and potassium therapy in multifocal atrial tachycardia. Am Heart J. 1985;110:789-794.http://www.ncbi.nlm.nih.gov/pubmed/4050650?tool=bestpractice.com
宽QRS波群(>120ms)伴室律规则
房性心动过速、心房扑动和常见室上性心动过速如果伴有差异性传导,则可出现左束支传导阻滞或右束支传导阻滞的心电图改变。这是宽QRS波心动过速鉴别诊断的重要部分。
特发性室性心动过速(心脏结构正常的单形性室速):
反复单形性室速也称为右室流出道心动过速 [Figure caption and citation for the preceding image starts]: 右心室流出道室性心动过速资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].由于主要起源于右室流出道,因此被认为是触发活动引起的局灶性心律失常。病因学未明,最常见于心脏结构正常的中青年患者,多由运动、情绪波动、应激或激素波动诱发。[15]Deal BJ, Miller SM, Scagliotti D, et al. Ventricular tachycardia in a young population without overt heart disease. Circulation. 1986;73:1111-1118.http://circ.ahajournals.org/cgi/reprint/73/6/1111http://www.ncbi.nlm.nih.gov/pubmed/3698245?tool=bestpractice.com较少见的起源部位有:左室流出道,左室心外膜,肺动脉瓣上或二尖瓣环室间隔面。源于这些区域的室速与右室流出道室速相似,都表现为良性的临床过程。
[Figure caption and citation for the preceding image starts]: 右心室流出道室性心动过速资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].由于主要起源于右室流出道,因此被认为是触发活动引起的局灶性心律失常。病因学未明,最常见于心脏结构正常的中青年患者,多由运动、情绪波动、应激或激素波动诱发。[15]Deal BJ, Miller SM, Scagliotti D, et al. Ventricular tachycardia in a young population without overt heart disease. Circulation. 1986;73:1111-1118.http://circ.ahajournals.org/cgi/reprint/73/6/1111http://www.ncbi.nlm.nih.gov/pubmed/3698245?tool=bestpractice.com较少见的起源部位有:左室流出道,左室心外膜,肺动脉瓣上或二尖瓣环室间隔面。源于这些区域的室速与右室流出道室速相似,都表现为良性的临床过程。
特发性左室型室性心动过速是由于围绕特殊传导组织和慢钙离子敏感心肌组织的折返引起,病因学不明。该心律失常对钙离子拮抗剂敏感,可被终止与控制。折返环常涉及左后分支,因此12-导联心电图上室速QRS波群相对较窄,呈右束支传导阻滞图形,电轴上偏。该类型室速见于年龄在15-40岁心脏结构正常的患者,其中70%为男性。此类室性心动过速多与猝死风险增加无关。[16]Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Circulation. 2006;114:e385-e484.http://circ.ahajournals.org/content/114/10/e385.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/16935995?tool=bestpractice.com
加速性心室自主节律:自发起搏灶源于心室肌,与室性心动过速类似,室率不快于窦性心律的20%(80-120次/分)。[16]Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Circulation. 2006;114:e385-e484.http://circ.ahajournals.org/content/114/10/e385.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/16935995?tool=bestpractice.com
单形性室速与既往心肌梗死有关:心律失常通常源于健康心肌与受损心肌交界区,以折返性心律最多见。[17]de Bakker JM, van Capelle FJ, Janse MJ, et al. Reentry as a cause of ventricular tachycardia in patients with chronic ischemic heart disease: electrophysiologic and anatomic correlation. Circulation. 1988;77:589-606.http://circ.ahajournals.org/cgi/reprint/77/3/589http://www.ncbi.nlm.nih.gov/pubmed/3342490?tool=bestpractice.com更常见于大面积心肌梗死和心功能降低的患者。
与非缺血性心肌病相关的单形性室性心动过速:不管心肌病病因如何,心室肌内传导的异质性是发生折返的基础,导致临床上室性心动过速发作。某些特殊型的心肌病值得特别关注。[16]Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Circulation. 2006;114:e385-e484.http://circ.ahajournals.org/content/114/10/e385.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/16935995?tool=bestpractice.com
致心律失常性右室发育不良:特征是右室脂肪浸润、纤维化和心室变薄,由此引起的折返导致室性心动过速。 [Figure caption and citation for the preceding image starts]: 致心律失常性右室心肌病患者伴发室性心动过速资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 致心律失常性右室心肌病患者伴发室性心动过速资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].
束支折返性室性心动过速:非缺血性扩张型心肌病患者发生持续性室速的常见类型。折返环往往向前传导至右束支,跨过室间隔,并沿左束支逆向传导。发作期间,12-导联心电图的特点是呈左束支传导阻滞图形。
结节性心肌病:结节影响20%-30%的心肌,心肌呈现片状肉芽肿、纤维化和疤痕,这是导致室性心动过速的病理基础。
Chagas心肌病:室性心动过速主要见于慢性Chagas心肌病,可能源于克氏锥虫感染引起的自身免疫反应。其机制很可能与导致的心肌纤维化有关。室性心动过速是在此病理基础上发生折返所致。
快速房性心律失常与附加旁路有关:任何房性心律失常(房扑,室上速)经由希氏-浦肯野系统正常传导,表现为窄QRS波群,如果存在有关附加旁路,则呈现宽QRS波群心动过速。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com [Figure caption and citation for the preceding image starts]: 室上性心动过速伴差传资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].另外,并存快速室上性节律时,仅于心动过速时发生室率相关的束支阻滞,从而形成宽QRS心动过速形态。
[Figure caption and citation for the preceding image starts]: 室上性心动过速伴差传资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].另外,并存快速室上性节律时,仅于心动过速时发生室率相关的束支阻滞,从而形成宽QRS心动过速形态。 [Figure caption and citation for the preceding image starts]: 频率依赖性左束支传导阻滞资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 频率依赖性左束支传导阻滞资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].
逆向型房室折返性心动过速: [Figure caption and citation for the preceding image starts]: 逆行性折返性心动过速资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].折返环内前向下传至附加旁路,逆向回至房室结,导致宽QRS波群形态。该型心律失常的折返环与顺向性房室折返性心动过速相同,但方向相反。鉴于激动经附加旁路前向下传,因此QRS波群呈现最大预激波。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com
[Figure caption and citation for the preceding image starts]: 逆行性折返性心动过速资料来源于医学博士 Robert W. Rho 的收集;经获准使用 [Citation ends].折返环内前向下传至附加旁路,逆向回至房室结,导致宽QRS波群形态。该型心律失常的折返环与顺向性房室折返性心动过速相同,但方向相反。鉴于激动经附加旁路前向下传,因此QRS波群呈现最大预激波。[1]Blomström-Lundqvist C, Scheinman M, Aliot EM, et al. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias. J Am Coll Cardiol. 2003;42:1493-1531.http://www.sciencedirect.com/science/article/pii/S0735109703011410http://www.ncbi.nlm.nih.gov/pubmed/14563598?tool=bestpractice.com
起搏心律:安装起搏器的患者由于快速心室起搏可呈宽QRS波。最常见的情况是,双腔起搏器感知到房性心律失常(房性心动过速和心房颤动)而随后引起快速心室起搏。
宽QRS波(>120ms)伴不规则心室率
原因如下:
QRS间期多变伴不规则心室率
多形性室速伴正常QT间期:最常见于急性冠状动脉综合征或心肌缺血,也见于心脏结构正常的患者。心肌梗死时发生多形性室速提示缺血持续进展,应针对基本缺血进行处理。离子通道病可出现多形性室速。儿茶酚胺敏感多形性室速发生于心脏结构症儿童或青少年患者,常表现为应激或运动诱发的晕厥或猝死。业已鉴定出多种基因与其有关,心脏ryanodine受体基因常染色体显性遗传突变是其中之一。[18]Passman R, Kadish A. Polymorphic ventricular tachycardia, long Q-T syndrome, and torsades de pointes. Med Clin North Am. 2001;85:321-341.http://www.ncbi.nlm.nih.gov/pubmed/11233951?tool=bestpractice.com与之相关的还有心脏calsequestrin基因常染色体隐性突变,但较少见。这些基因突变能造成肌质网钙释放。[19]The Cardiac Society of Australia and New Zealand. Guidelines for the diagnosis and management of catecholaminergic polymorphic ventricular tachycardia. 2011. http:// www.csanz.edu.au/ (last accessed 19 August 2016).http://www.csanz.edu.au/wp-content/uploads/2013/11/Diagnosis-and-Management-of-CPVT.pdf
尖端扭转型室性心动过速:多形性室速伴有QT间期延长(窦性节律时可观察到),其特征是QRS波群绕等电位线连续扭转。QT延长可以是先天性或获得性原因。临床上,获得性长QT综合征较常见,这可能继发于使用某些延长QT间期的药物、AZCERT: QT drugs list 缺血、显著电解质紊乱(低钾血症,低镁血症,低钙血症)、或中枢神经系统的重大创伤。[18]Passman R, Kadish A. Polymorphic ventricular tachycardia, long Q-T syndrome, and torsades de pointes. Med Clin North Am. 2001;85:321-341.http://www.ncbi.nlm.nih.gov/pubmed/11233951?tool=bestpractice.com
双向室性心动过速:很罕见,是致命性心律失常。 最多见于洋地黄中毒,也见于儿茶酚胺敏感多形性室速和Anderson-Tawil综合征(长QT6)。其特征是两种形态的QRS波群交替出现(常为右束支阻滞伴电轴左右交替)。这与心室二联律相反,双向VT的R-R间期是规则的。[16]Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Circulation. 2006;114:e385-e484.http://circ.ahajournals.org/content/114/10/e385.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/16935995?tool=bestpractice.com
心房颤动伴心室预激:存在前向传导附加旁路的房颤患者可以表现为宽QRS波不规则心动过速。在伴前向传导旁路的患者中,有些下传速率更快,因此发生心律失常风险较大。识别这种心律失常很关键,因为其可导致心室颤动和血流动力学崩溃。房颤伴预激是一种潜在性威胁生命的心律失常。[12]Fuster V, Ryden L, Cannom D, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation - executive summary. J Am Coll Cardiol. 2006;48:854-906.http://content.onlinejacc.org/article.aspx?articleid=1137853http://www.ncbi.nlm.nih.gov/pubmed/16904574?tool=bestpractice.com
心室颤动:室率快(>300次/分),节律极不规则和致命性的室性心律失常,QRS周期长度、形态和幅度多变。[16]Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Circulation. 2006;114:e385-e484.http://circ.ahajournals.org/content/114/10/e385.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/16935995?tool=bestpractice.com
