许多 PID 发作未被发现。[1]Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64:1-137.http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6403a1.htmhttp://www.ncbi.nlm.nih.gov/pubmed/26042815?tool=bestpractice.com尽管一些 PID 患者无症状,但另一些有症状未被诊断的病例(诸如异常阴道出血、性交痛和阴道分泌物异常)是因为患者或医疗保健提供者不能识别轻度或非特异性症状或体征。由于临床正确诊断PID比较困难,而临床症状轻微或无临床症状的 PID 对女性生殖健康可能造成潜在损伤,因此医疗保健提供者应降低 PID 的诊断阈值,尤其是在 PID 高危人群中(诸如 15-24 岁性活跃女性、STD 门诊患者以及居住在淋病或衣原体感染高发区域的人群)。[1]Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64:1-137.http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6403a1.htmhttp://www.ncbi.nlm.nih.gov/pubmed/26042815?tool=bestpractice.com[15]US Preventive Services Task Force. Screening for chlamydial infection: US
Preventive Services Task Force recommendation statement. Ann Intern Med. 2007;147:128-134.http://www.annals.org/content/147/2/128.longhttp://www.ncbi.nlm.nih.gov/pubmed/17576996?tool=bestpractice.com
病史
病史应侧重于识别 PID 的高危因素。衣原体或淋菌感染病史是 PID 最重要的高危因素。[6]Dayan L. Pelvic inflammatory disease. Aust Fam Physician. 2006;35:858-862.http://www.ncbi.nlm.nih.gov/pubmed/17099803?tool=bestpractice.com从病史得出的其他重要高危因素包括初次性交年龄小、与多名性伴侣无保护性交、PID 病史以及使用 IUD。[6]Dayan L. Pelvic inflammatory disease. Aust Fam Physician. 2006;35:858-862.http://www.ncbi.nlm.nih.gov/pubmed/17099803?tool=bestpractice.com[8]Holmes KK, Levine R, Weaver M. Effectiveness of condoms in preventing sexually transmitted infections. Bull World Health Organ. 2004;82:454-461.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2622864/?tool=pubmedhttp://www.ncbi.nlm.nih.gov/pubmed/15356939?tool=bestpractice.com[9]Ness RB, Randall H, Richter HE, et al. Pelvic Inflammatory Disease Evaluation and Clinical Health Study Investigators. Condom use and the risk of recurrent pelvic inflammatory disease, chronic pelvic pain, or infertility following an episode of pelvic inflammatory disease. Am J Public Health. 2004;94:1327-1329.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1448448/http://www.ncbi.nlm.nih.gov/pubmed/15284036?tool=bestpractice.com[10]McCormack, WM. Pelvic inflammatory disease. N Engl J Med. 1994;330:115-119.http://www.ncbi.nlm.nih.gov/pubmed/8259168?tool=bestpractice.com也应询问有无吸烟史、社会经济地位低、近期阴道冲洗以及经期性交等病史。PID 可引起各种各样的非特异性症状,尽管如此,这些症状的出现仍具有高度提示性,应加以了解:[16]British Association for Sexual Health and HIV. UK national guideline for the management of pelvic inflammatory disease. June 2011. http://www.bashh.org/guidelines (last accessed 16 March 2016).http://www.bashh.org/documents/3572.pdf
下腹痛,通常是双侧
恶心和呕吐
深部性交痛
异常阴道出血,包括性交后、经间期,以及月经过多
异常阴道或宫颈分泌物,通是脓性的。
体格检查
建议从常规检查开始进行系统的临床检查。常规检查应包括测定体温 (>38°C [>101°F])。对腹部的浅触诊和深触诊可以检查下腹部压痛,通常为双侧压痛。应进行盆腔检查,从外生殖器开始检查,查看有无异常阴道分泌物。随后进行窥器检查,暴露阴道和宫颈,查看子宫颈管有无黏液脓性或脓性分泌物。 [Figure caption and citation for the preceding image starts]: 衣原体感染引起的宫颈糜烂和红肿的体征CDC 图像库/Lourdes Fraw 博士,Jim Pledger;准许使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 衣原体感染引起的宫颈糜烂和红肿的体征CDC 图像库/Lourdes Fraw 博士,Jim Pledger;准许使用 [Citation ends].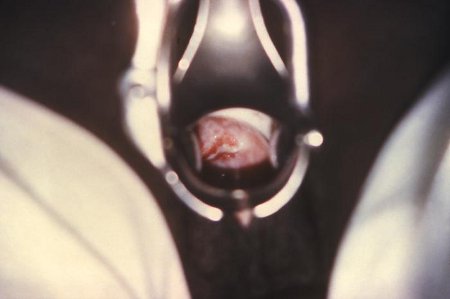 [Figure caption and citation for the preceding image starts]: 淋菌性宫颈炎CDC 图像库;准许使用 [Citation ends].然后进行双合诊检查,查看是否具备以下一个或多个最低诊断标准:
[Figure caption and citation for the preceding image starts]: 淋菌性宫颈炎CDC 图像库;准许使用 [Citation ends].然后进行双合诊检查,查看是否具备以下一个或多个最低诊断标准:
特别是对淋菌感染存在高风险的女性,应采用三个拭子(宫颈、尿道和直肠)收集标本。
初诊
一个或多个附加标准可增加最低诊断标准的特异性,有助于诊断 PID:[1]Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64:1-137.http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6403a1.htmhttp://www.ncbi.nlm.nih.gov/pubmed/26042815?tool=bestpractice.com
口腔温度>38.3°C (>101°F)
宫颈或阴道异常黏液脓性分泌物
阴道分泌物生理盐水显微镜检见到大量 白细胞
ESR 升高
C 反应蛋白升高
实验室证实的宫颈沙眼衣原体或淋病奈瑟球菌感染。
其他实验室检查
由于不正确的诊断和处理可能会导致不必要的发病率,因此经常需要更精细的诊断评估。当质疑诊断或者患者对治疗无效时,需要进一步的检查。虽有多个不同成本和可用的检查和程序,但没有一个单一的实验室检查是有诊断性的。不过,在这种情况下,血清白细胞计数、湿涂片多形核白细胞以及 血沉的正常结果可以有效地排除上生殖道感染。[3]Crossman SH. The challenge of pelvic inflammatory disease. Am Fam Physician. 2006;73:859-864.http://www.aafp.org/afp/2006/0301/p859.htmlhttp://www.ncbi.nlm.nih.gov/pubmed/16529095?tool=bestpractice.com[17]Peipert JF, Ness RB, Blume J, et al. Clinical predictors of endometritis in women with symptoms and signs of pelvic inflammatory disease. Am J Obstet Gynecol. 2001;184:856-863.http://www.ncbi.nlm.nih.gov/pubmed/11303192?tool=bestpractice.com 在初诊时应考虑这些检查。
影像学和侵入性检查
对临床诊断不能确诊的患者以及那些病情严重或对初次治疗无效的患者可采用影像学检查。影像学检查包括经阴道超声、CT 和 MRI。每项检查都显示 PID 的特征性表现。
经阴道超声是主要的影像学检查方式,在早期或无并发症病例,检查结果可能是正常的。使用彩色或能量多普勒可增加较轻微的子宫内膜炎、输卵管炎和卵巢炎的检出率。[18]Horrow MM. Ultrasound of pelvic inflammatory disease. Ultrasound Q. 2004;2:171-179.http://www.ncbi.nlm.nih.gov/pubmed/15602219?tool=bestpractice.com
弥漫性盆腔痛、腹膜炎、或者超声诊断困难或不明确的患者需要做盆腔 CT。由于未显影的肠管可能会被误认为是脓肿,所以均应口服和静脉注射造影剂。[19]Vandermeer FQ, Wong-You-Cheong JJ. Imaging of acute pelvic pain. Clin Obstet
Gynecol. 2009;52:2-20.http://www.ncbi.nlm.nih.gov/pubmed/19179858?tool=bestpractice.com
在诊断输卵管卵巢脓肿、输卵管积脓、输卵管积液和/或有游离盆腔积液的较大多囊卵巢的患者时,盆腔 MRI优于超声。然而,超声和 CT 的成本费用要低于 MRI。因此,很少使用MRI,只起到一个补充性的解决问题的作用。[19]Vandermeer FQ, Wong-You-Cheong JJ. Imaging of acute pelvic pain. Clin Obstet
Gynecol. 2009;52:2-20.http://www.ncbi.nlm.nih.gov/pubmed/19179858?tool=bestpractice.com
腹腔镜可以直接从输卵管和道格拉斯陷凹收集样本,当质疑诊断时,在排除其他病变时特别有用。腹腔镜不能检查子宫内膜炎或轻度输卵管炎。它不能用作常规诊断工具,尤其当症状轻微或不明显时。[1]Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64:1-137.http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6403a1.htmhttp://www.ncbi.nlm.nih.gov/pubmed/26042815?tool=bestpractice.com
子宫内膜活检不应作为常规诊断试验。对腹腔镜检查无输卵管炎证据的女性,建议使用子宫内膜活检。[1]Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64:1-137.http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6403a1.htmhttp://www.ncbi.nlm.nih.gov/pubmed/26042815?tool=bestpractice.com
经验性治疗
对性活跃的年轻女性和其他具有 PID 高危因素的女性(例如 15-24 岁的女性;来自PID高发社区[按患病率升高定义]的女性;有个体危险因素的女性[例如近来多个性伴侣、STD 病史、性伴侣患有 STD];以及那些与外界隔绝、商业性交易或吸毒有关的女性),初诊时应开始经验性治疗。[1]Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64:1-137.http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6403a1.htmhttp://www.ncbi.nlm.nih.gov/pubmed/26042815?tool=bestpractice.com[15]US Preventive Services Task Force. Screening for chlamydial infection: US
Preventive Services Task Force recommendation statement. Ann Intern Med. 2007;147:128-134.http://www.annals.org/content/147/2/128.longhttp://www.ncbi.nlm.nih.gov/pubmed/17576996?tool=bestpractice.com由于 PID 未及时治疗可造成严重健康隐患以及对侵入性检查缺乏清晰的时间界定,建议医生对有下腹部压痛、附件区压痛、或宫颈举痛的患病危险的患者开始治疗。90% 以上的腹腔镜检确诊的病例中都有这些体检发现。[10]McCormack, WM. Pelvic inflammatory disease. N Engl J Med. 1994;330:115-119.http://www.ncbi.nlm.nih.gov/pubmed/8259168?tool=bestpractice.com
