乳头状、滤泡性或Hurthle细胞性
对于大多数患者,标准的治疗方案是先手术,术后行放射性碘消融以及TSH抑制治疗。
全甲状腺切除有利于术后进行放射性碘扫描寻找可能的转移灶,并且有利于随访过程中对甲状腺球蛋白水平的监测。 乳头状癌也可能为多中心性。 对于存在任何不良预后因素,比如男性、老年、结节较大或生长较快等,全甲状腺切除是必要的。[6]Cobin RH, Gharib H, Bergman DA, et al; Thyroid Carcinoma Task Force. AACE/AAES medical/surgical guidelines for clinical practice: management of thyroid carcinoma. Endocr Pract. 2001 May-Jun;7(3):202-20.http://www.aace.com/files/thyroid-carcinoma.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/11430305?tool=bestpractice.com 分化型甲状腺癌的分期系统是基于美国癌症协会(AJCC)系统以及转移、年龄、完整切除、侵袭、肿瘤大小(MACIS)等因素制定的。[30]Lang BH, Lo CY, Chan WF, et al. Staging systems for papillary thyroid carcinoma: a review and comparison. Ann Surg. 2007 Mar;245(3):366-78.http://www.ncbi.nlm.nih.gov/pubmed/17435543?tool=bestpractice.com[31]Lang BH, Lo CY, Chan WF, et al. Staging systems for follicular thyroid carcinoma: application to 171 consecutive patients treated in a tertiary referral centre. Endocr Relat Cancer. 2007 Mar;14(1):29-42.http://www.ncbi.nlm.nih.gov/pubmed/17395973?tool=bestpractice.com 甲状腺半切除术(腺叶及峡部切除,术后TSH抑制)适用于单侧的分化性癌、结节<1cm、没有不良预后因素的患者。[16]Gharib H, Papini E, Garber JR, et al. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules - 2016 update. Endocr Pract. 2016;22(Suppl 1):1-60.http://journals.aace.com/doi/pdf/10.4158/EP161208.GLhttp://www.ncbi.nlm.nih.gov/pubmed/27167915?tool=bestpractice.com 在全甲状腺切除时,气管前淋巴结需一并切除。[34]White ML, Gauger PG, Doherty GM, et al. Central lymph node dissection in differentiated thyroid cancer. World J Surg. 2007 May;31(5):895-904.http://www.ncbi.nlm.nih.gov/pubmed/17347896?tool=bestpractice.com 有淋巴结病变的患者需行单侧选择性颈清扫。 预防性中央区清扫仍存在争议。 一些中心推荐行中央区清扫,但是缺乏明确证据可改善预后,比如对于复发和死亡的获益。[35]Shan CX, Zhang W, Jiang DZ, et al. Routine central neck dissection in differentiated thyroid carcinoma: a systematic review and meta-analysis. Laryngoscope. 2012 Apr;122(4):797-804.http://www.ncbi.nlm.nih.gov/pubmed/22294492?tool=bestpractice.com[36]Zetoune T, Keutgen X, Buitrago D, et al. Prophylactic central neck dissection and local recurrence in papillary thyroid cancer: a meta-analysis. Ann Surg Oncol. 2010 Dec;17(12):3287-93.http://www.ncbi.nlm.nih.gov/pubmed/20596784?tool=bestpractice.com[37]Hughes DT, Doherty GM. Central neck dissection for papillary thyroid cancer. Cancer Control. 2011 Apr;18(2):83-8.http://www.ncbi.nlm.nih.gov/pubmed/21451450?tool=bestpractice.com 常规伤口引流并没有改善恢复效果,比如避免术后积液,却延长了患者住院时间。[38]Samraj K, Gurusamy KS. Wound drains following thyroid surgery. Cochrane Database Syst Rev. 2007;(4):CD006099.http://www.ncbi.nlm.nih.gov/pubmed/17943885?tool=bestpractice.com
全甲状腺切除术后可能出现一些并发症,其中喉返神经损伤或甲状旁腺功能减退的风险为2%。[6]Cobin RH, Gharib H, Bergman DA, et al; Thyroid Carcinoma Task Force. AACE/AAES medical/surgical guidelines for clinical practice: management of thyroid carcinoma. Endocr Pract. 2001 May-Jun;7(3):202-20.http://www.aace.com/files/thyroid-carcinoma.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/11430305?tool=bestpractice.com 全甲状腺切除术后发生永久性甲状旁腺功能减退的概率高于次全切除。 需要经验丰富的外科医生来完成此手术。
有些患者细针穿刺提示滤泡性肿瘤而接受了甲状腺半切除术,而最终病理证实为滤泡癌。 细针穿刺无法可靠地鉴别良性(腺瘤)和恶性(癌)滤泡性肿瘤,即使冰冻切片也可能无法明确鉴别。 有以下三种治疗选择:
治疗决策基于临床评估以及与乳头状癌相同的预后危险因素。[39]Inabnet WB. Surgical management of thyroid cancer. Endocr Pract. 2000 Nov-Dec;6(6):465-8.http://www.ncbi.nlm.nih.gov/pubmed/11155221?tool=bestpractice.com
初始治疗后,I-131 可清除检测到的复发病灶或转移病灶。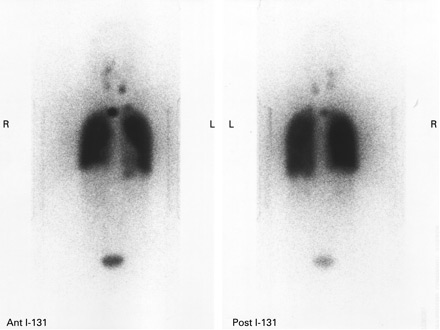 [Figure caption and citation for the preceding image starts]: 甲状腺乳头状癌肺转移病灶为粟粒状,表现为肺内及纵隔内放射性碘浓聚。Gkountouvas A, Chatjimarkou F, Thomas D, et al. Miliary lung metastasis due to papillary thyroid carcinoma. BMJ Case Reports. 2009; doi:10.1136/bcr.06.2008.0322 [Citation ends]. 分化性甲状腺癌已行全甲状腺切除的患者,如何选择一个合适的剂量,是放射性碘治疗成败的关键。 一项研究显示,对术后残留病灶的消除,3700MBq的高剂量比1110MBq的低剂量更为有效。[40]Fallahi B, Beiki D, Takavar A, et al. Low versus high radioiodine dose in postoperative ablation of residual thyroid tissue in patients with differentiated thyroid carcinoma: a large randomized clinical trial. Nucl Med Commun. 2012 Mar;33(3):275-82.http://www.ncbi.nlm.nih.gov/pubmed/22124360?tool=bestpractice.com 另一项研究则指出,低剂量I-131联合促甲状腺素α与高剂量I-131效果相似,且副作用较少。[41]Mallick U, Harmer C, Yap B, et al. Ablation with low-dose radioiodine and thyrotropin alfa in thyroid cancer. New Engl J Med. 2012 May 3;366(18):1674-85.http://www.nejm.org/doi/full/10.1056/NEJMoa1109589#t=articlehttp://www.ncbi.nlm.nih.gov/pubmed/22551128?tool=bestpractice.com 如果颈部的复发或转移病灶可通过手术评估,那么也可以通过手术切除。 TSH抑制治疗需要一直持续。 对于绝经后没有使用雌激素的女性,骨质流失是潜在的后遗症。[2]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133.http://online.liebertpub.com/doi/pdf/10.1089/thy.2015.0020http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com[42]Sugitani I, Fujimoto Y. Effect of postoperative thyrotropin suppressive therapy on bone mineral density in patients with papillary thyroid carcinoma: a prospective controlled study. Surgery. 2011 Dec;150(6):1250-7.http://www.ncbi.nlm.nih.gov/pubmed/22136848?tool=bestpractice.com 但是,TSH抑制治疗导致骨折的风险尚不清楚。心血管疾病、心律失常、或骨折的风险:一项大样本队列观察研究所得的中等质量的证据显示,与非抑制性TSH治疗相比,抑制性TSH治疗可能使这些风险增加。[43]Flynn RW, Bonellie SR, Jung RT, et al. Serum thyroid-stimulating hormone concentration and morbidity from cardiovascular disease and fractures in patients on long-term thyroxine therapy. J Clin Endocrinol Metab. 2010;95:186-193.http://www.ncbi.nlm.nih.gov/pubmed/19906785?tool=bestpractice.com受试者<200名的随机对照临床试验(RCT)、受试者>200名且方法学存在缺陷的随机对照临床试验(RCT)、方法学存在缺陷的系统评价或者高质量的观察性(队列)研究。
[Figure caption and citation for the preceding image starts]: 甲状腺乳头状癌肺转移病灶为粟粒状,表现为肺内及纵隔内放射性碘浓聚。Gkountouvas A, Chatjimarkou F, Thomas D, et al. Miliary lung metastasis due to papillary thyroid carcinoma. BMJ Case Reports. 2009; doi:10.1136/bcr.06.2008.0322 [Citation ends]. 分化性甲状腺癌已行全甲状腺切除的患者,如何选择一个合适的剂量,是放射性碘治疗成败的关键。 一项研究显示,对术后残留病灶的消除,3700MBq的高剂量比1110MBq的低剂量更为有效。[40]Fallahi B, Beiki D, Takavar A, et al. Low versus high radioiodine dose in postoperative ablation of residual thyroid tissue in patients with differentiated thyroid carcinoma: a large randomized clinical trial. Nucl Med Commun. 2012 Mar;33(3):275-82.http://www.ncbi.nlm.nih.gov/pubmed/22124360?tool=bestpractice.com 另一项研究则指出,低剂量I-131联合促甲状腺素α与高剂量I-131效果相似,且副作用较少。[41]Mallick U, Harmer C, Yap B, et al. Ablation with low-dose radioiodine and thyrotropin alfa in thyroid cancer. New Engl J Med. 2012 May 3;366(18):1674-85.http://www.nejm.org/doi/full/10.1056/NEJMoa1109589#t=articlehttp://www.ncbi.nlm.nih.gov/pubmed/22551128?tool=bestpractice.com 如果颈部的复发或转移病灶可通过手术评估,那么也可以通过手术切除。 TSH抑制治疗需要一直持续。 对于绝经后没有使用雌激素的女性,骨质流失是潜在的后遗症。[2]Haugen BR, Alexander EK, Bible KC, et al; American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2016 Jan;26(1):1-133.http://online.liebertpub.com/doi/pdf/10.1089/thy.2015.0020http://www.ncbi.nlm.nih.gov/pubmed/26462967?tool=bestpractice.com[42]Sugitani I, Fujimoto Y. Effect of postoperative thyrotropin suppressive therapy on bone mineral density in patients with papillary thyroid carcinoma: a prospective controlled study. Surgery. 2011 Dec;150(6):1250-7.http://www.ncbi.nlm.nih.gov/pubmed/22136848?tool=bestpractice.com 但是,TSH抑制治疗导致骨折的风险尚不清楚。心血管疾病、心律失常、或骨折的风险:一项大样本队列观察研究所得的中等质量的证据显示,与非抑制性TSH治疗相比,抑制性TSH治疗可能使这些风险增加。[43]Flynn RW, Bonellie SR, Jung RT, et al. Serum thyroid-stimulating hormone concentration and morbidity from cardiovascular disease and fractures in patients on long-term thyroxine therapy. J Clin Endocrinol Metab. 2010;95:186-193.http://www.ncbi.nlm.nih.gov/pubmed/19906785?tool=bestpractice.com受试者<200名的随机对照临床试验(RCT)、受试者>200名且方法学存在缺陷的随机对照临床试验(RCT)、方法学存在缺陷的系统评价或者高质量的观察性(队列)研究。
对于放射性碘难治性转移性分化性甲状腺癌, 已有全身性治疗,如索拉非尼和乐伐替尼。 这两种激酶抑制剂都可改善结局;但是毒性也很明显。[44]Brose MS, Nutting CM, Jarzab B, et al; DECISION Investigators. Sorafenib in radioactive iodine-refractory, locally advanced or metastatic differentiated thyroid cancer: a randomised, double-blind, phase 3 trial. Lancet. 2014 Jul 26;384(9940):319-28.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4366116/http://www.ncbi.nlm.nih.gov/pubmed/24768112?tool=bestpractice.com[45]Schlumberger M, Tahara M, Wirth LJ, et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N Engl J Med. 2015 Feb 12;372(7):621-30.http://www.nejm.org/doi/full/10.1056/NEJMoa1406470#t=articlehttp://www.ncbi.nlm.nih.gov/pubmed/25671254?tool=bestpractice.com 因此,索拉菲尼和仑伐替尼应仅用于有明确疾病进展证据且毒性可控的患者。[44]Brose MS, Nutting CM, Jarzab B, et al; DECISION Investigators. Sorafenib in radioactive iodine-refractory, locally advanced or metastatic differentiated thyroid cancer: a randomised, double-blind, phase 3 trial. Lancet. 2014 Jul 26;384(9940):319-28.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4366116/http://www.ncbi.nlm.nih.gov/pubmed/24768112?tool=bestpractice.com[45]Schlumberger M, Tahara M, Wirth LJ, et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N Engl J Med. 2015 Feb 12;372(7):621-30.http://www.nejm.org/doi/full/10.1056/NEJMoa1406470#t=articlehttp://www.ncbi.nlm.nih.gov/pubmed/25671254?tool=bestpractice.com
髓样癌
甲状腺髓样癌的手术方式为全甲状腺切除。 没有可疑淋巴病变的患者需接受中央区淋巴结清扫。 如果有淋巴病变(临床查体、影像学、或术中探查)且组织学证实为转移(细针穿刺或冰冻切片)的,需要接受病变侧改良根治性颈淋巴结清扫。
髓样癌的遗传易感者(多发性内分泌肿瘤MEN或家族性综合征)需要接受预防性全甲状腺切除。
复发患者可再次行手术治疗,对局部控制欠佳的患者需辅以放疗。
对于进展期甲状腺髓样癌,凡德他尼,一种口服的多靶点酪氨酸激酶抑制剂,与安慰剂相比可显示一定的疗效。[46]Wells SA Jr, Robinson BG, Gagel RF, et al. Vandetanib in patients with locally advanced or metastatic medullary thyroid cancer: a randomized, double-blind phase III trial. J Clin Oncol. 2012 Jan 10;30(2):134-41.http://ascopubs.org/doi/full/10.1200/jco.2011.35.5040http://www.ncbi.nlm.nih.gov/pubmed/22025146?tool=bestpractice.com[47]Frampton JE. Vandetanib: in medullary thyroid cancer. Drugs. 2012 Jul 9;72(10):1423-36.http://www.ncbi.nlm.nih.gov/pubmed/22715896?tool=bestpractice.com无进展生存:一项针对331例局部进展或转移性甲状腺髓样癌患者的随机(2:1)双盲对照研究所得的高质量的证据显示,与安慰剂相比,凡德他尼可明显延长无进展生存时间(危险比:0.46;95%CI 0.31-0.69;p<0.001),中位随访时间为24个月。[46]Wells SA Jr, Robinson BG, Gagel RF, et al. Vandetanib in patients with locally advanced or metastatic medullary thyroid cancer: a randomized, double-blind phase III trial. J Clin Oncol. 2012 Jan 10;30(2):134-41.http://ascopubs.org/doi/full/10.1200/jco.2011.35.5040http://www.ncbi.nlm.nih.gov/pubmed/22025146?tool=bestpractice.com系统评价或者受试者>200名的随机对照临床试验(RCT)。 凡德他尼适用于局部侵袭性或有症状的进展、或者远处转移、且无法接受手术治疗的甲状腺髓样癌患者。 其禁忌症包括长QT综合征。
左甲状腺素仅用于甲状腺切除后的替代治疗,不作为对潜在恶性肿瘤的治疗,因为髓样癌对促甲状腺激素 (TSH) 不敏感。[6]Cobin RH, Gharib H, Bergman DA, et al; Thyroid Carcinoma Task Force. AACE/AAES medical/surgical guidelines for clinical practice: management of thyroid carcinoma. Endocr Pract. 2001 May-Jun;7(3):202-20.http://www.aace.com/files/thyroid-carcinoma.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/11430305?tool=bestpractice.com 因此,给予左甲状腺素的抑制剂量是不必要的。
