特发性颅内高压 (IIH) 是一种以意识清醒患者颅内压增高伴相关体征和症状为特征的综合征,但无局灶性神经症状。[1]Wall M. Idiopathic intracranial hypertension. Neurol Clin. 2010;28:593-617.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2908600/http://www.ncbi.nlm.nih.gov/pubmed/20637991?tool=bestpractice.com 除了脑脊液 (CSF) 压力增加以外,没有脑室系统畸形或阻塞的证据,神经诊断学检查均正常。 此外,颅内高压无明显继发性原因。 该疾病可以是自限性的,也可发展为终身性慢性病。[1]Wall M. Idiopathic intracranial hypertension. Neurol Clin. 2010;28:593-617.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2908600/http://www.ncbi.nlm.nih.gov/pubmed/20637991?tool=bestpractice.com
应询问患者的临床表现包括头痛、肩部和颈部疼痛、脉搏同步耳鸣、短暂性视力障碍、畏光、视力缺失和复视。
检查时可能发现的体征包括视盘水肿、第六神经麻痹以及感官视觉功能障碍。普遍存在视野缺损,早期缺损的标准模式表现为盲点扩大和鼻下视野缺损。[30]Keltner JL, Johnson CA, Cello KE, et al. Baseline visual field findings in the Idiopathic Intracranial Hypertension Treatment Trial (IIHTT). Invest Ophthalmol Vis Sci. 2014 Apr 29;55(5):3200-7.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4031894/http://www.ncbi.nlm.nih.gov/pubmed/24781936?tool=bestpractice.com 目前可用的诊断标准为改良的 Dandy 标准。[31]Smith JL. Whence pseudotumor cerebri? J Clin Neuroophthalmol. 1985 Mar;5(1):55-6.http://www.ncbi.nlm.nih.gov/pubmed/3156890?tool=bestpractice.com[32]Frisen L. Swelling of the optic nerve head: a staging scheme. J Neurol Neurosurg Psychiatry. 1982 Jan;45(1):13-8.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC491259/pdf/jnnpsyc00045-0021.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/7062066?tool=bestpractice.com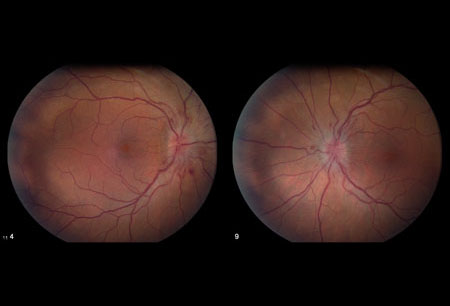 [Figure caption and citation for the preceding image starts]: 双侧乳头水肿来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 双侧乳头水肿来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].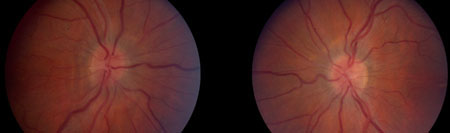 [Figure caption and citation for the preceding image starts]: 双侧神经盘肿胀消退来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 双侧神经盘肿胀消退来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].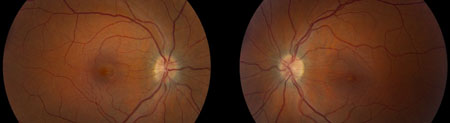 [Figure caption and citation for the preceding image starts]: 双侧视神经萎缩来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 双侧视神经萎缩来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].
病史
应考虑下列疾病史,因为它们可能导致颅内压增高:
通过蛛网膜颗粒的血流量减少:之前炎症引起的疤痕(例如继发于蛛网膜下腔出血的脑膜炎)。
静脉回流受阻:静脉窦血栓(高凝状态、连续感染(例如,中耳或乳突 - 耳炎性脑积水)、双侧根治性颈清扫术、上腔静脉综合征或右心压力增加)。
内分泌失调:原发性慢性肾上腺皮质功能减退症、甲状旁腺功能减退、皮质类固醇戒断
营养失调:维生素 A 过多症(摄入维生素、肝脏或异维 A 酸)、母爱剥夺性侏儒营养过度
动静脉畸形和硬脑膜分流。
还应询问的其他可能原因以确定不存在可能致病的历史因素:
临床特征
患者可能出现头痛、颈部和肩部疼痛、短暂性视力障碍、脉冲同步性耳鸣、畏光和眼球后疼痛。 复视和视力缺失不太常见。 有些症状在对照组中也较为常见,所以很少根据单一症状而诊断为 IIH。 脉搏同步性耳鸣很少见于对照组,所以可作为颅内压增高的相对特异性症状。
头痛:患者普遍存在,是常见症状。 症状可能包括每天严重搏动性头痛。[33]Wall M. The headache profile of idiopathic intracranial hypertension. Cephalalgia. 1990 Dec;10(6):331-5.http://www.ncbi.nlm.nih.gov/pubmed/2289234?tool=bestpractice.com 患者可被头痛唤醒,且通常持续几个小时。患者通常报告该头痛是他们经历过的最严重的头部疼痛。常见恶心,但呕吐较少见。不存在 IIH 的典型头痛,但它通常表现为日常的全头颅性头痛。许多患者都有混合性头痛综合征,包括偏头痛和镇痛药过量性头痛。一项研究对特发性颅内压增高症治疗临床试验中的头痛进行分析,得出的结论为,头痛可能主要与脑脊液压力增高以外的因素有关,提示需给予特异性的头痛治疗。[34]Friedman DI, Quiros PA, Subramanian PS, el al. Headache in idiopathic intracranial hypertension: Findings from the Idiopathic Intracranial Hypertension Treatment Trial. Headache. 2017 Sep;57(8):1195-1205.http://www.ncbi.nlm.nih.gov/pubmed/28752894?tool=bestpractice.com
短暂性视力障碍:短暂性灰视或视野昏暗,通常持续时间不超过 30 秒,之后会恢复。 大约四分之三患者会出现视力障碍。[35]Giuseffi V, Wall M, Siegel PZ, et al. Symptoms and disease associations in idiopathic intracranial hypertension (pseudotumor cerebri): a case-control study. Neurology. 1991 Feb;41(2 ( Pt 1)):239-44.http://www.ncbi.nlm.nih.gov/pubmed/1992368?tool=bestpractice.com 发作可呈单眼性或双眼性。 目前认为以上症状是由组织压力增加,导致视神经头短暂性缺血而引起的。[36]Sadun AA, Currie JN, Lessell S. Transient visual obscurations with elevated optic discs. Ann Neurol. 1984 Oct;16(4):489-94.http://www.ncbi.nlm.nih.gov/pubmed/6497356?tool=bestpractice.com 虽然一些研究未能表明,短暂性视力障碍的出现可能与视力不佳结局有关,[37]Bulens C, Meerwaldt JD, Koudstaal PJ, et al. Spatial contrast sensitivity in benign intracranial hypertension. J Neurol Neurosurg Psychiatry. 1988 Oct;51(10):1323-9.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1032922/pdf/jnnpsyc00545-0075.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/3225588?tool=bestpractice.com[38]Corbett JJ. The 1982 Silversides lecture: problems in the diagnosis and treatment of pseudotumor cerebri. Can J Neurol Sci. 1983 Nov;10(4):221-9.http://www.ncbi.nlm.nih.gov/pubmed/6652584?tool=bestpractice.com[39]Rush JA. Pseudotumor cerebri: clinical profile and visual outcome in 63 patients. Mayo Clin Proc. 1980 Sep;55(9):541-6.http://www.ncbi.nlm.nih.gov/pubmed/7412408?tool=bestpractice.com一项研究发现,频繁的暂时性视力模糊(每日超过一次)是视力结局差的一个危险因素。[40]Wall M, Falardeau J, Fletcher WA, et al. Risk factors for poor visual outcome in patients with idiopathic intracranial hypertension. Neurology. 2015 Sep 1;85(9):799-805.http://www.ncbi.nlm.nih.gov/pubmed/26245929?tool=bestpractice.com
脉冲同步耳鸣:约 60% 的患者会发生该症状。[35]Giuseffi V, Wall M, Siegel PZ, et al. Symptoms and disease associations in idiopathic intracranial hypertension (pseudotumor cerebri): a case-control study. Neurology. 1991 Feb;41(2 ( Pt 1)):239-44.http://www.ncbi.nlm.nih.gov/pubmed/1992368?tool=bestpractice.com 多为单侧性耳鸣,左侧和右侧的发生率相同。 颅内压增高的患者,颈静脉加压与耳鸣同侧。[41]Meador KJ, Swift TR. Tinnitus from intracranial hypertension. Neurology. 1984 Sep;34(9):1258-61.http://www.ncbi.nlm.nih.gov/pubmed/6540416?tool=bestpractice.com 通常认为耳鸣是由增强的血管搏动的传输导致的,静脉造影时可见塌陷的横静脉窦狭窄(引起血流紊流);它是 ICP 升高的相对特异性症状。
检查
医生应评估是否存在视神经乳头水肿及相关性视力缺失和第六颅神经麻痹。 如果存在其他神经系统检查异常,应强烈怀疑 IIH 以外的其他诊断。
眼底检查:视神经乳头水肿是 IIH 的基本标志,但必须与假性视神经乳头水肿进行鉴别。 无论是直接的还是间接的视神经乳头水肿,都会导致视力缺失。 在一般情况下,视神经乳头水肿的等级越高,视力丧失越严重。[14]Wall M, White WN 2nd. Asymmetric papilledema in idiopathic intracranial hypertension: prospective interocular comparison of sensory visual function. Invest Ophthalmol Vis Sci. 1998 Jan;39(1):134-42.http://www.iovs.org/content/39/1/134.full.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/9430554?tool=bestpractice.com 用改良 Frisén 分级量表对视神经乳头水肿进行分级,以密切注意患者并确定视力不良结局的风险。[42]Scott CJ, Kardon RH, Lee AG, et al. Diagnosis and grading of papilledema in patients with raised intracranial pressure using optical coherence tomography vs clinical expert assessment using a clinical staging scale. Arch Ophthalmol. 2010 Jun;128(6):705-11.http://www.ncbi.nlm.nih.gov/pubmed/20547947?tool=bestpractice.com 但是,针对个体患者,很难通过视盘水肿的严重程度预测视力缺失的严重程度。一种可能的解释是:随着视神经压迫导致的轴突死亡,视盘水肿程度会减轻。神经纤维层出血与治疗结局较差有关。[43]Wall M, Thurtell MJ; NORDIC Idiopathic Intracranial Hypertension Study Group. Optic disc haemorrhages at baseline as a risk factor for poor outcome in the Idiopathic Intracranial Hypertension Treatment Trial. Br J Ophthalmol. 2017 Sep;101(9):1256-60.http://www.ncbi.nlm.nih.gov/pubmed/28130349?tool=bestpractice.com
眼球运动障碍:约 33% 患者会发生水平复视,10% 至 20% 患者会出现第六颅神经麻痹。[44]Wall M, George D. Idiopathic intracranial hypertension. A prospective study of 50 patients. Brain. 1991 Feb;114 (pt 1A):155-80.http://www.ncbi.nlm.nih.gov/pubmed/1998880?tool=bestpractice.com 也有针对第六颅神经麻痹以外的其他运动功能障碍的相关报告。 其中一些是因为轻微垂直眼部运动失调(伴随第六颅神经麻痹出现)而得出的错误结论。 对于患有眼部运动失调而没有第六颅神经麻痹的患者,应对其 IIH 诊断持怀疑态度。
感官视觉功能:视神经乳头水肿患者的视敏度通常是正常或接近正常的,除非长期患病和病情严重。 Snellen 视敏度轻度丧失的情况并不少见,[45]NORDIC Idiopathic Intracranial Hypertension Study Group; Wall M, Kupersmith MJ, Kieburtz KD, et al. The idiopathic intracranial hypertension treatment trial: clinical profile at baseline. JAMA Neurol. 2014 Jun;71(6):693-701.http://archneur.jamanetwork.com/article.aspx?articleid=1861749http://www.ncbi.nlm.nih.gov/pubmed/24756302?tool=bestpractice.com 但该检测对判断视野测量时视力丧失的范围和视盘水肿的恶化程度不具有敏感性。[44]Wall M, George D. Idiopathic intracranial hypertension. A prospective study of 50 patients. Brain. 1991 Feb;114 (pt 1A):155-80.http://www.ncbi.nlm.nih.gov/pubmed/1998880?tool=bestpractice.com 对比敏感度测试更敏感,但如果已经进行了适当的视野测量,该测试通常是多余的。
视野测量:IIH 患者在视野测量时普遍出现视力缺失。视力丧失:低质量证据表明,除了生理盲点扩大以外,>90% 的患者至少一只眼睛经 Goldmann 视野测量发现视力丧失,自动视野测量的结果相似。[44]Wall M, George D. Idiopathic intracranial hypertension. A prospective study of 50 patients. Brain. 1991 Feb;114 (pt 1A):155-80.http://www.ncbi.nlm.nih.gov/pubmed/1998880?tool=bestpractice.com低质量的观察性(队列)研究或者受试者<200名且方法学存在缺陷的随机对照临床试验(RCT)。 其中约四分之一为轻度视力丧失,患者很少察觉。[44]Wall M, George D. Idiopathic intracranial hypertension. A prospective study of 50 patients. Brain. 1991 Feb;114 (pt 1A):155-80.http://www.ncbi.nlm.nih.gov/pubmed/1998880?tool=bestpractice.com
该病的视野缺损与其他原因所致视盘水肿的视野缺损属同一类型,而且与青光眼患者所见视盘水肿相似。最常见的缺损是生理盲点增大和鼻下部分视野缺损,[30]Keltner JL, Johnson CA, Cello KE, et al. Baseline visual field findings in the Idiopathic Intracranial Hypertension Treatment Trial (IIHTT). Invest Ophthalmol Vis Sci. 2014 Apr 29;55(5):3200-7.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4031894/http://www.ncbi.nlm.nih.gov/pubmed/24781936?tool=bestpractice.com 伴等视力线收缩。中央缺陷明显较为少见,除非出现高度视盘水肿导致的大量浆液性视网膜脱离,否则需要考虑其他诊断。视野损失可能较为严重,并呈进行性加重,可导致失明。视力缺失通常是随时间推移逐渐进展的。但是,缺血性视神经病变时可见急性严重性视力缺失。
盲点扩大十分常见。 因为折射常常会消除这种缺损,所以除非其影响不会减轻不应认为出现显著的视力缺失。 后者通常是神经上皮脱离导致的,光学相干断层扫描 (OCT) 下最易发现。 另外,因为盲点的大小与折射密切相关,所以不能将其用于疗程跟踪。 盲点附近区域出现轻度视力缺失,也可能因脉络膜皱褶而发生。 因为视野内存在视力丧失(主要是在外围),所以视野平均偏差(整体视力丧失的指标)是用于以下患者的良好衡量标准。[46]Wall M, Johnson CA, Cello KE, et al. Visual Field Outcomes for the Idiopathic Intracranial Hypertension Treatment Trial (IIHTT). Invest Ophthalmol Vis Sci. 2016 Mar;57(3):805-12.http://iovs.arvojournals.org/article.aspx?articleid=2499292http://www.ncbi.nlm.nih.gov/pubmed/26934136?tool=bestpractice.com
检查
所有患者应进行以下检查。
Snellen 视敏度检查:视神经乳头水肿患者的视敏度通常是正常或接近正常的,除非长期患病、病情严重或存在神经上皮脱离。 Snellen 视敏度轻度丧失的情况并不少见,[45]NORDIC Idiopathic Intracranial Hypertension Study Group; Wall M, Kupersmith MJ, Kieburtz KD, et al. The idiopathic intracranial hypertension treatment trial: clinical profile at baseline. JAMA Neurol. 2014 Jun;71(6):693-701.http://archneur.jamanetwork.com/article.aspx?articleid=1861749http://www.ncbi.nlm.nih.gov/pubmed/24756302?tool=bestpractice.com 但该检测对判断视野测量时视力丧失的范围和视盘水肿的恶化程度不具有敏感性。[44]Wall M, George D. Idiopathic intracranial hypertension. A prospective study of 50 patients. Brain. 1991 Feb;114 (pt 1A):155-80.http://www.ncbi.nlm.nih.gov/pubmed/1998880?tool=bestpractice.com
相对性传入性瞳孔反应障碍 (RAPD):一项评估传入通路疾病的客观性测试。 可通过中性密度滤光装置来量化缺陷程度。
眼球运动检查:评估眼球运动缺陷,包括第六颅神经麻痹。
自动静态或 Goldmann(动态)视野测量:用于检查盲点扩大、鼻下视野缺损、其他神经纤维束缺损或视野收缩。
视神经乳头成像或 Frisén 分级:应根据改良后的 Frisén 视神经乳头水肿量表分析视神经乳头成像。[42]Scott CJ, Kardon RH, Lee AG, et al. Diagnosis and grading of papilledema in patients with raised intracranial pressure using optical coherence tomography vs clinical expert assessment using a clinical staging scale. Arch Ophthalmol. 2010 Jun;128(6):705-11.http://www.ncbi.nlm.nih.gov/pubmed/20547947?tool=bestpractice.com[32]Frisen L. Swelling of the optic nerve head: a staging scheme. J Neurol Neurosurg Psychiatry. 1982 Jan;45(1):13-8.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC491259/pdf/jnnpsyc00045-0021.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/7062066?tool=bestpractice.com [Figure caption and citation for the preceding image starts]: Frisén 1 级来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: Frisén 1 级来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].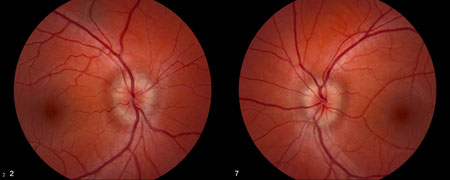 [Figure caption and citation for the preceding image starts]: Frisén 2 级来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: Frisén 2 级来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].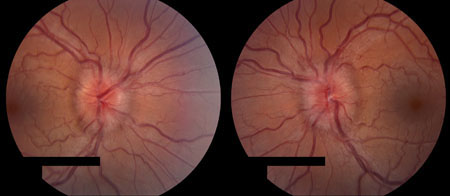 [Figure caption and citation for the preceding image starts]: Frisén 3 级来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: Frisén 3 级来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends]. [Figure caption and citation for the preceding image starts]: Frisén 4 级来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: Frisén 4 级来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].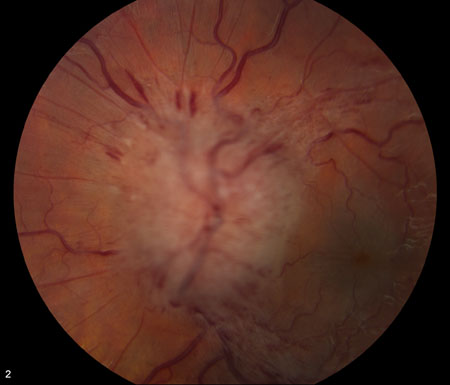 [Figure caption and citation for the preceding image starts]: Frisén 5 级来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: Frisén 5 级来自 M. Wall 医生个人收集的资料;获准使用 [Citation ends].
造影或未造影的大脑磁共振成像 (MRI):寻找眶内和颅内病变。 需要轴状面和矢状面图来评估空泡蝶鞍。
腰椎穿刺:排除颅内占位性病变后可进行。 局麻后在腰椎 L3/L4 间隙进行无菌穿刺,测量开口压力前,患者左侧卧位,腿伸直,保持正常呼吸频率和深度(没有明显的过度通气或通气不足)。 患者坐立时,穿刺针更容易进入蛛网膜下腔,然后让患者保持侧卧位,测量压力,采集脑脊液。
磁共振静脉造影:用于检查双边横窦静脉狭窄;静脉窦血栓的检查结果为阴性。
除了脑脊液测压时出现颅内压增高以外,实验室检查结果是正常的。 如存在异常神经影像学结果(除了空泡蝶鞍,未折叠的视神经纤维髓壳和侧窦部分塌陷),应考虑其他诊断。
脑脊液压力升高
关于脑脊液开放压力的测量标准,存在几个问题。 测量的参考水平应是左心房的水平,无论患者仰卧还是俯卧或坐位。 应当指出的是,捏鼻鼓气和通气不足(与镇静作用有关的)时可能会出现假性高值。[47]Neville L, Egan RA. Frequency and amplitude of elevation of cerebrospinal fluid resting pressure by the Valsalva maneuver. Can J Ophthalmol. 2005 Dec;40(6):775-7.http://www.ncbi.nlm.nih.gov/pubmed/16391647?tool=bestpractice.com 儿童尤其容易反复出现通气不足的问题。 实际上,因二氧化碳水平下降,过度通气的焦急患者也可出现假性低值。[48]Lim MJ, Lin JP. The effects of carbon dioxide on measuring cerebral spinal fluid pressure. Childs Nerv Syst. 2009 Jul;25(7):783-4.http://www.ncbi.nlm.nih.gov/pubmed/19452156?tool=bestpractice.com
脑脊液开放压力的正常限值仍然存在争议。 非肥胖者的正常范围是< 200 mm H2O,但对于肥胖患者,存在许多相互冲突的研究。[49]Bono F, Quattrone A. CSF opening pressure: reference interval and the effect of body mass index. Neurology. 2007 Apr 24;68(17):1439-40.http://www.ncbi.nlm.nih.gov/pubmed/17452597?tool=bestpractice.com[50]Corbett JJ, Mehta MP. Cerebrospinal fluid pressure in normal obese subjects and patients with pseudotumor cerebri. Neurology. 1983 Oct;33(10):1386-8.http://www.ncbi.nlm.nih.gov/pubmed/6684240?tool=bestpractice.com[51]Whiteley W, Al-Shahi R, Warlow CP, et al. CSF opening pressure: reference interval and the effect of body mass index. Neurology. 2006 Nov 14;67(9):1690-1.http://www.ncbi.nlm.nih.gov/pubmed/17101909?tool=bestpractice.com 体重指数 (BMI) 增加会使脑脊液压力轻度增加。[52]Berdahl JP, Fleischman D, Zaydlarova J, et al. Body mass index has a linear relationship with cerebrospinal fluid pressure. Invest Ophthalmol Vis Sci. 2012 Mar 15;53(3):1422-7.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3339912/http://www.ncbi.nlm.nih.gov/pubmed/22323469?tool=bestpractice.com 200 mm H2O 至 250 mm H2O 被认为是边界值,超过 250 mm H2O 一定属于脑脊液压力升高。 在儿童和青少年中,该值应>280 mm H2O。[53]Avery RA, Shah SS, Licht DJ, et al. Reference range for cerebrospinal fluid opening pressure in children. N Engl J Med. 2010 Aug 26;363(9):891-3.http://www.nejm.org/doi/full/10.1056/NEJMc1004957http://www.ncbi.nlm.nih.gov/pubmed/20818852?tool=bestpractice.com
进行多针穿刺的患者,其结果可能会假性偏低。 相反,单次测量可能是有误导性的,因为腰椎穿刺测量的脑脊液压力只能代表一个时间点的压力,而脑脊液压力是在一整天内波动的,甚至有时 IIH 患者的测量结果是正常的。 因此,脑脊液单次测量值正常并不能排除 IIH 的诊断,单次压力测量在改良治疗方面的临床使用很有限。 重复腰椎穿刺(以前作为 IIH 的一种治疗方法)也会增加患椎管内表皮样肿瘤的风险(表皮细胞植入导致的)。[54]Batnitzky S, Keucher TR, Mealey J Jr, et al. Iatrogenic intraspinal epidermoid tumors. JAMA. 1977 Jan 10;237(2):148-50.http://www.ncbi.nlm.nih.gov/pubmed/576154?tool=bestpractice.com
光学相干断层扫描 (OCT)
这是一种用于测量视网膜神经纤维层厚度和发现视神经乳头水肿进展的影像学检查技术。[42]Scott CJ, Kardon RH, Lee AG, et al. Diagnosis and grading of papilledema in patients with raised intracranial pressure using optical coherence tomography vs clinical expert assessment using a clinical staging scale. Arch Ophthalmol. 2010 Jun;128(6):705-11.http://www.ncbi.nlm.nih.gov/pubmed/20547947?tool=bestpractice.com
