卒中的首发症状存在很大差异,具体取决于卒中的发病机制、体积和部位。快速评估和诊断性检查对鉴别缺血性卒中与出血性卒中,从而启动恰当的管理至关重要。出血性卒中的最高危险因素包括:慢性高血压、男性;黑人/西班牙裔血统;出血性卒中家族史;高龄;遗传性毛细血管扩张症;血友病;COL4A1、KRIT1、CCM2 或 PDCD10 基因的常染色体显性突变;使用抗凝治疗;可卡因滥用;血管畸形;以及脑淀粉样血管病。
初始评估
初始评估包括对气道(呼吸、脉搏血氧测定、口腔分泌物积聚)和循环(血压、血管通路)的评估。在稳定病情的同时或稳定后即刻,进行卒中发病症状的病史采集和精简的神经系统体格检查。美国国立卫生研究院卒中量表 (NIHSS) 是临床试验中常用的卒中征象快速体格评估工具,也可用于临床实践中。
美国国立卫生研究院 (NIH) 卒中量表
脑出血 (ICH) 评分是使用最为广泛的疾病严重程度分级量表,可在 ICH 发生后早期预测结局。ICH 评分要素包括:ICH 量(>30 cm² = 1 分);格拉斯哥昏迷评分(3-4 = 2 分,5-12 = 1 分)、是否有脑室内出血(是 = 1)、ICH 是否位于幕下(是 = 1 分)以及年龄(>80 岁 = 1 分)。[16]Hemphill JC 3rd, Bonovich DC, Besmertis L, et al. The ICH score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke. 2001 Apr;32(4):891-7.https://www.ahajournals.org/doi/full/10.1161/01.str.32.4.891http://www.ncbi.nlm.nih.gov/pubmed/11283388?tool=bestpractice.com 其他有用的量表还有格拉斯哥昏迷量表 (Glasgow Coma Scale, GCS) 和原发性脑出血患者神经功能结局预测量表(FUNC 评分)。Massachusetts General Hospital Stroke Service: FUNC score calculator 尽管这些量表用作正式的预后情况评估工具,但一项研究结果显示,比起 ICH 和 FUNC 评分,医生的早期主观判断与 3 个月时的结局更具紧密相关性。[37]Hwang DY, Dell CA, Sparks MJ, et al. Clinician judgment vs formal scales for predicting intracerebral hemorrhage outcomes. Neurology. 2016 Jan 12;86(2):126-33.http://www.ncbi.nlm.nih.gov/pubmed/26674335?tool=bestpractice.com既往史可以帮助判断患者是否存在与凝血功能损害有关的疾病,例如肝病和血液病等。完整的用药史对于诊断患者是否为与抗凝药物相关的出血很重要。几项观察性研究提示,常规使用非甾体抗炎药 (NSAIDs) 可能增加心血管事件的发病率以及增加卒中风险。然而,在对观察性研究进行的一项 meta 分析中,认为非甾体抗炎药作为一个单独的类别与出血性卒中的风险显著增加不相关,但在使用特定药物(双氯芬酸和美洛昔康)的患者中,观察到风险显著增加。[31]Ungprasert P, Matteson EL, Thongprayoon C. Nonaspirin nonsteroidal anti-inflammatory drugs and risk of hemorrhagic stroke: a systematic review and meta-analysis of observational studies. Stroke. 2016 Feb;47(2):356-64.http://www.ncbi.nlm.nih.gov/pubmed/26670086?tool=bestpractice.com 尽管一项使用最大剂量阿托伐他汀的随机临床试验显示,治疗组发生出血性卒中的风险更高,且独立于胆固醇降低的程度,[38]Iso H, Jacobs DR Jr, Wentworth D, et al. Serum cholesterol levels and six-year mortality from stroke in 350,977 men screened for the multiple risk factor intervention trial. N Engl J Med. 1989 Apr 6;320(14):904-10.http://www.ncbi.nlm.nih.gov/pubmed/2619783?tool=bestpractice.com[39]Amarenco P, Bogousslavsky J, Callahan A 3rd, et al; The Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators. High-dose atorvastatin after stroke or transient ischemic attack. N Engl J Med. 2006 Aug 10;355(6):549-59.https://www.nejm.org/doi/full/10.1056/NEJMoa061894http://www.ncbi.nlm.nih.gov/pubmed/16899775?tool=bestpractice.com 但已证实他汀类药物并不增加出血的风险;此外,有研究发现,入院前服用他汀类药物的颅内出血患者预后更佳。[40]McKinney JS, Kostis WJ. Statin therapy and the risk of intracerebral hemorrhage: a meta-analysis of 31 randomized controlled trials. Stroke. 2012 Aug;43(8):2149-56.http://www.ncbi.nlm.nih.gov/pubmed/22588266?tool=bestpractice.com[41]Biffi A, Devan WJ, Anderson CD, et al. Statin use and outcome after intracerebral hemorrhage: case-control study and meta-analysis. Neurology. 2011 May 3;76(18):1581-8.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3100126/http://www.ncbi.nlm.nih.gov/pubmed/21451150?tool=bestpractice.com 此外,研究显示在急性脑内出血时,最初 ICH 量或 24 小时血肿量的增加与使用他汀类药物之间并无关系。[42]Priglinger M, Arima H, Anderson C, et al; INTERACT Investigators. No relationship of lipid-lowering agents to hematoma growth: pooled analysis of the intensive blood pressure reduction in acute cerebral hemorrhage trials studies. Stroke. 2015 Mar;46(3):857-9.https://www.ahajournals.org/doi/full/10.1161/strokeaha.114.007664http://www.ncbi.nlm.nih.gov/pubmed/25657175?tool=bestpractice.com[43]Ma Y, Li Z, Chen L, et al. Blood lipid levels, statin therapy and the risk of intracerebral hemorrhage. Lipids Health Dis. 2016 Mar 1;15:43.https://lipidworld.biomedcentral.com/articles/10.1186/s12944-016-0213-8http://www.ncbi.nlm.nih.gov/pubmed/26932585?tool=bestpractice.com
在大多数情况下,脑出血患者的症状在数秒至数分钟内发生进展,最常见的症状包括:
四肢无力
感觉异常或麻木
头晕
眩晕
恶心/呕吐
言语困难
视觉缺损或复视
意识错乱
头痛。
脑出血的首发体征各有不同,取决于出血的脑区。[44]Passero S, Rocchi R, Rossi S, et al. Seizures after spontaneous supratentorial intracerebral hemorrhage. Epilepsia. 2002 Oct;43(10):1175-80.http://www.ncbi.nlm.nih.gov/pubmed/12366733?tool=bestpractice.com 发生出血时可伴发癫痫发作。[44]Passero S, Rocchi R, Rossi S, et al. Seizures after spontaneous supratentorial intracerebral hemorrhage. Epilepsia. 2002 Oct;43(10):1175-80.http://www.ncbi.nlm.nih.gov/pubmed/12366733?tool=bestpractice.com 神经系统体格检查最常见的体征包括:
尚无可靠的体征能有效地鉴别缺血性卒中和脑出血;但相对而言,脑出血患者更常出现意识水平下降和颅内压增高的体征。脑干和小脑位置的出血较缺血性卒中而言,发生意识水平改变、昏迷和呕吐的情况更为常见。
后续检测
脑部成像
必须鉴别缺血性卒中与出血性卒中。由于许多神经系统疾病与卒中相似,因此,我们必须明确诊断。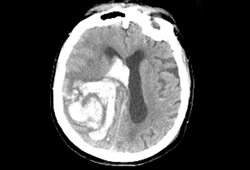 [Figure caption and citation for the preceding image starts]: 颅内出血的 CT 表现麻省总医院 (Massachusetts General Hospital) 患者个人病历档案;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 颅内出血的 CT 表现麻省总医院 (Massachusetts General Hospital) 患者个人病历档案;经许可后使用 [Citation ends].
如果已经明确脑出血,我们需要进一步关注出血的部位和形状,以及是否存在如动静脉畸形 (arteriovenous malformation, AVM)、肿瘤或脑梗死等相关病变,这些信息有助于明确是否为继发性出血性卒中及其可能的病因。
由于 CT 血管造影能快速排除动静脉畸形 (AVM) 或血管瘤等继发性病因的存在,部分中心联合进行计算机体层成像 (CT) 检查和 CT 血管造影。此外,注射后 CT 影像上显示血肿床内有高密度对比剂(斑点征)与之后血肿扩张的风险较高。[45]Wada R, Aviv RI, Fox AJ, et al. CT angiography "spot sign" predicts hematoma expansion in acute intracerebral hemorrhage. Stroke. 2007 Apr;38(4):1257-62.https://www.ahajournals.org/doi/full/10.1161/01.str.0000259633.59404.f3http://www.ncbi.nlm.nih.gov/pubmed/17322083?tool=bestpractice.com[46]Goldstein JN, Fazen LE, Snider R, et al. Contrast extravasation on CT angiography predicts hematoma expansion in intracerebral hemorrhage. Neurology. 2007 Mar 20;68(12):889-94.http://www.ncbi.nlm.nih.gov/pubmed/17372123?tool=bestpractice.com 点征评分能帮助预测血肿的进展和不良临床预后的可能性。[47]Delgado Almandoz JE, Yoo AJ, Stone MJ, et al. Systematic characterization of the computed tomography angiography spot sign in primary intracerebral hemorrhage identifies patients at highest risk for hematoma expansion: the spot sign score. Stroke. 2009 Sep;40(9):2994-3000.https://www.ahajournals.org/doi/full/10.1161/strokeaha.109.554667http://www.ncbi.nlm.nih.gov/pubmed/19574553?tool=bestpractice.com[48]Almandoz JE, Yoo AJ, Stone MJ, et al. The spot sign score in primary intracerebral hemorrhage identifies patients at highest risk of in-hospital mortality and poor outcome among survivors. Stroke. 2010 Jan;41(1):54-60.http://www.ncbi.nlm.nih.gov/pubmed/19910545?tool=bestpractice.com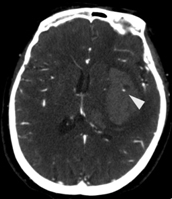 [Figure caption and citation for the preceding image starts]: CTA 图像上存在点征(箭头所示处)说明在造影后 CT 图像上血肿内部存在高密度造影剂;通常认为这样的患者之后出现血肿进展的可能性更大。山麓医疗中心 (Foothills Medical Center) 患者个人病历档案;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: CTA 图像上存在点征(箭头所示处)说明在造影后 CT 图像上血肿内部存在高密度造影剂;通常认为这样的患者之后出现血肿进展的可能性更大。山麓医疗中心 (Foothills Medical Center) 患者个人病历档案;经许可后使用 [Citation ends].
考虑到血肿频繁扩大,在诊断 CT 后,应当最好至少再做一次脑部影像学检查,用以评估扩大情况并确定最终的血肿大小。[49]Naidech AM. Diagnosis and management of spontaneous intracerebral hemorrhage. Continuum (Minneap Minn). 2015 Oct;21(5 Neurocritical Care):1288-98.http://www.ncbi.nlm.nih.gov/pubmed/26426231?tool=bestpractice.com
血液检查和心电图检查
建议进行其他检查明确病因。识别潜在病因非常重要,因为颅内出血幸存者发生后续颅内出血的可能性高于后续缺血性卒中或心肌梗死。[50]Bailey RD, Hart RG, Benavente O, et al. Recurrent brain hemorrhage is more frequent than ischemic stroke after intracranial hemorrhage. Neurology. 2001 Mar 27;56(6):773-7.http://www.ncbi.nlm.nih.gov/pubmed/11274313?tool=bestpractice.com
血管成像
当动脉瘤破裂且主要表现为脑实质出血时,有必要进行血管影像检查,以排除 AVM 或其他罕见疾病。[51]Zhu XL, Chan MS, Poon WS. Spontaneous intracranial hemorrhage: which patients need diagnostic cerebral angiography? A prospective study of 206 cases and review of the literature. Stroke. 1997 Jul;28(7):1406-9.https://www.ahajournals.org/doi/full/10.1161/01.str.28.7.1406http://www.ncbi.nlm.nih.gov/pubmed/9227692?tool=bestpractice.com 建议以下人群进行检查:1)所有<45 岁的患者;2)脑叶出血的患者;3)根据出血位置判断出血可能为脑静脉窦/静脉血栓所致的患者;4)考虑伴有动脉瘤破裂引发的蛛网膜下腔出血患者。
检查手段包括:传统的有创血管造影、CTA 和磁共振血管造影 (MRA)。传统的有创血管造影能检测到无创检查可能遗漏的小 AVM,但由于有创检查的安全性问题,现已被无创检查所取代。较 MRA 而言,CTA 的空间分辨率更高,因此在两者皆可行的情况下,医生们更倾向于进行 CTA 检查。当高度怀疑患者存在 AVM 时,即使无创血管检查影像未见异常,仍建议进行传统的有创血管造影明确诊断。
磁共振成像(MRI)
当需要与某些疾病(例如血管畸形、肿瘤或脑静脉窦/静脉血栓)进行鉴别诊断时,建议采用 MRI 检查。MRI 可以检测出一些继发性出血病因,例如血管成像无法显示的海绵状血管畸形、肿瘤和 CT 图像中并不十分明显的脑梗塞病灶。[2]Smith EE, Rosand J, Greenberg SM. Hemorrhagic stroke. Neuroimaging Clin N Am. 2005 May;15(2):259-72.http://www.ncbi.nlm.nih.gov/pubmed/16198939?tool=bestpractice.com
出血灶中的铁质具有磁敏感效应,梯度回波 (GRE) 序列能敏感地检测出这一效应,因而被广泛地用于检查患者是否存在微出血。如果患者无其他可能病因,且仅脑叶存在多发微出血,提示患者可能患有脑淀粉样血管病。[8]Smith EE, Greenberg SM. Clinical diagnosis of cerebral amyloid angiopathy: validation of the Boston criteria. Curr Atheroscler Rep. 2003 Jul;5(4):260-6.http://www.ncbi.nlm.nih.gov/pubmed/12793966?tool=bestpractice.com 因脑淀粉样血管病所致的原发性脑出血复发出血的风险高,故较其他病因所致的脑出血预后更差,及时诊断具有重要意义。[52]Viswanathan A, Rakich SM, Engel C, et al. Antiplatelet use after intracerebral hemorrhage. Neurology. 2006 Jan 24;66(2):206-9.http://www.ncbi.nlm.nih.gov/pubmed/16434655?tool=bestpractice.com 磁敏感加权成像 (SWI) 是一种较新的 MRI 成像技术。与 MRI GRE 序列相比,SWI 能更为敏感地诊断微出血和微小脑海绵状血管畸形。[53]Mittal S, Wu Z, Neelavalli J, et al. Susceptibility-weighted imaging: technical aspects and clinical applications, part 2. AJNR Am J Neuroradiol. 2009 Feb;30(2):232-52.http://www.ajnr.org/content/30/2/232.fullhttp://www.ncbi.nlm.nih.gov/pubmed/19131406?tool=bestpractice.com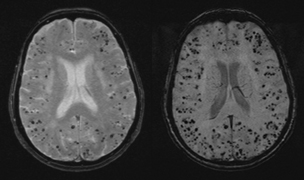 [Figure caption and citation for the preceding image starts]: 左图是一位 80 岁女性患者的 MRI GRE 序列图像,其上存在许多点状低信号(黑点),提示患者可能患有脑淀粉样血管病,导致脑叶多发微出血。而右图为同一患者的 MRI SWI 序列图像,从中我们可以看到很多并未在 GRE 序列上显示的微出血灶。山麓医疗中心 (Foothills Medical Center) 患者个人病历档案;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 左图是一位 80 岁女性患者的 MRI GRE 序列图像,其上存在许多点状低信号(黑点),提示患者可能患有脑淀粉样血管病,导致脑叶多发微出血。而右图为同一患者的 MRI SWI 序列图像,从中我们可以看到很多并未在 GRE 序列上显示的微出血灶。山麓医疗中心 (Foothills Medical Center) 患者个人病历档案;经许可后使用 [Citation ends].
尚未有人研究过 MRI 的成本效益和诊断价值,但当需要鉴别诊断类似的高危疾病时,建议进行 MRI 检查。
 静脉穿刺和抽血的动画演示
静脉穿刺和抽血的动画演示
 关于如何进行心电图的动画演示
关于如何进行心电图的动画演示
