RAS 评估包括考虑患者病史中的因素和对合适影像学模式的确定。
病史
高血压发病的年龄可提示 RAS 的潜在病因:
年龄在 30 岁以下可提示有肌纤维发育不良 (FMD)。[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.[14]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:1425-1443.http://circ.ahajournals.org/content/127/13/1425.longhttp://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com
年龄在 55 岁以上可提示有动脉粥样硬化性 RAS。[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.[14]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:1425-1443.http://circ.ahajournals.org/content/127/13/1425.longhttp://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com
突然或不明原因的反复肺水肿是 RAS 的表征:[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.[14]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:1425-1443.http://circ.ahajournals.org/content/127/13/1425.longhttp://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com[15]Tendera M, Aboyans V, Bartelink ML, et al; European Stroke Organisation Authors/Task Force Members. ESC guidelines on the diagnosis and treatment of peripheral artery diseases. Eur Heart J. 2011;32:2851-2906.http://eurheartj.oxfordjournals.org/content/32/22/2851http://www.ncbi.nlm.nih.gov/pubmed/21873417?tool=bestpractice.com[16]Davenport A, Anker SD, Mebazaa A, et al.; Acute Dialysis Quality Initiative (ADQI) Consensus Group. ADQI 7: the clinical management of the Cardio-Renal syndromes: work group statements from the 7th ADQI consensus conference. Nephrol Dial Transplant. 2010;25:2077-2089.https://academic.oup.com/ndt/article/25/7/2077/1874047/ADQI-7-the-clinical-management-of-the-Cardio-Renalhttp://www.ncbi.nlm.nih.gov/pubmed/20494894?tool=bestpractice.com
高血压(急进性、恶性或难治性)
患有动脉粥样硬化或 FMD 型 RAS 的患者都会表现出严重的、进展性的和/或难以控制的高血压,有时会导致终末器官损害。[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.[14]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:1425-1443.http://circ.ahajournals.org/content/127/13/1425.longhttp://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com
肾功能不全或急性肾损伤:
原因不明的肾功能不全可能由进展性狭窄或高血压有关的终末器官损害所致。[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006;113:e463-e654.http://circ.ahajournals.org/content/113/11/e463.longhttp://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.
对于一些双侧 RAS 或开始使用血管紧张素转换酶抑制剂或血管紧张素 II 受体拮抗剂后的单个正常肾的 RAS 患者,会出现急性肾损伤。[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006;113:e463-e654.http://circ.ahajournals.org/content/113/11/e463.longhttp://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.
诱发动脉粥样硬化 RAS 的病史因素包括:[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006;113:e463-e654.http://circ.ahajournals.org/content/113/11/e463.longhttp://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com
多支冠状动脉疾病 (CAD)
其他外周血管疾病 (PVD)
不明原因的充血性心力衰竭
难治性心绞痛
血脂异常
吸烟(导致动脉粥样硬化性和 FMD 类型 RAS 的病因)[1]Safian RD, Textor SC. Renal-artery stenosis. N Engl J Med. 2001;344:431-442.http://www.ncbi.nlm.nih.gov/pubmed/11172181?tool=bestpractice.com[11]Slovut DP, Olin JW. Fibromuscular dysplasia. N Engl J Med. 2004;350:1862-1871.http://www.ncbi.nlm.nih.gov/pubmed/15115832?tool=bestpractice.com
无高血压家族史 - 可能提示 RAS 是高血压的病因。[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006;113:e463-e654.http://circ.ahajournals.org/content/113/11/e463.longhttp://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com[12]Eisenhauer AC, White CJ. Endovascular treatment of noncoronary obstructive vascular disease. In: Libby P, Bonow RO, Mann DL, et al., eds. Braunwald's heart disease. 8th ed. Philadelphia, PA: Elsevier Saunders; 2008:1532-1535.
检查
鉴于 RAS 只能采用影像学检查确诊,提示性的检查结果包括:
血压测量结果为高血压
腹部血管杂音:检查发现腹部血管杂音时应怀疑是否存在 RAS。[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006;113:e463-e654.http://circ.ahajournals.org/content/113/11/e463.longhttp://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.
其他杂音:由于常见的病理生理学因素和伴发 PVD 的高发病率,其他血管的杂音非常常见。[12]Eisenhauer AC, White CJ. Endovascular treatment of noncoronary obstructive vascular disease. In: Libby P, Bonow RO, Mann DL, et al., eds. Braunwald's heart disease. 8th ed. Philadelphia, PA: Elsevier Saunders; 2008:1532-1535.
一般性检查
检测血清肌酐以评估 GFR。[1]Safian RD, Textor SC. Renal-artery stenosis. N Engl J Med. 2001;344:431-442.http://www.ncbi.nlm.nih.gov/pubmed/11172181?tool=bestpractice.com
血清钾:低钾血症或低到正常钾可能提示肾素-血管紧张素-醛固酮系统活化。[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.
尿液分析和沉积物评估(排除肾小球疾病):在没有并发糖尿病性肾病或高血压性肾硬化的情况下,RAS 通常为非蛋白尿,且尿沉淀物中没有异常。[4]Chonchol M, Linas S. Diagnosis and management of ischemic nephropathy. Clin J Am Soc Nephrol. 2006;1:172-181.http://cjasn.asnjournals.org/content/1/2/172.fullhttp://www.ncbi.nlm.nih.gov/pubmed/17699206?tool=bestpractice.com[17]Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002;13(suppl 3):S184-S186.http://jasn.asnjournals.org/content/13/suppl_3/S184.fullhttp://www.ncbi.nlm.nih.gov/pubmed/12466311?tool=bestpractice.com
根据指征,应在鉴别诊断中排除和考虑对高血压继发性病因的评估:例如,醛固酮肾素比值(比值小于 20 应排除原发性醛固酮增多症)。[7]Kaplan NM. Renovascular hypertension. In: Kaplan NM, ed. Clinical hypertension. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2002:381-403.
影像学检查的选择
除了基本的实验室数据,对于采用何种影像学模式最为合适仍然存在争议。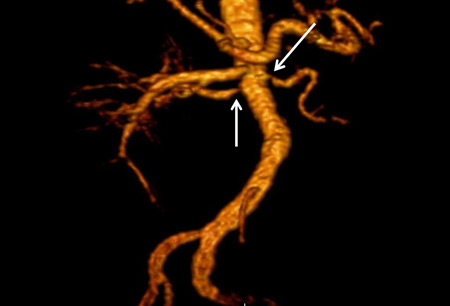 [Figure caption and citation for the preceding image starts]: 一位显著双侧动脉粥样硬化性肾动脉狭窄患者的磁共振血管造影(三维容积再现重建)。箭头指示近端双侧狭窄感谢马萨诸塞大学医疗中心和医学院放射科的 David J. Sheehan DO 的支持 [Citation ends].
[Figure caption and citation for the preceding image starts]: 一位显著双侧动脉粥样硬化性肾动脉狭窄患者的磁共振血管造影(三维容积再现重建)。箭头指示近端双侧狭窄感谢马萨诸塞大学医疗中心和医学院放射科的 David J. Sheehan DO 的支持 [Citation ends]. [Figure caption and citation for the preceding image starts]: 一位肾动脉肌纤维发育不良患者的磁共振血管造影(最大强度投影)。箭头指示右侧肾动脉出现特征性的不规则轮廓感谢哈佛医学院布里格姆妇科医院放射科 Raul Galvez MD MPH 和 Hale Ersoy MD 的支持 [Citation ends].
[Figure caption and citation for the preceding image starts]: 一位肾动脉肌纤维发育不良患者的磁共振血管造影(最大强度投影)。箭头指示右侧肾动脉出现特征性的不规则轮廓感谢哈佛医学院布里格姆妇科医院放射科 Raul Galvez MD MPH 和 Hale Ersoy MD 的支持 [Citation ends]. [Figure caption and citation for the preceding image starts]: 一位显著动脉粥样硬化性左肾动脉狭窄患者的数字减影血管造影。A 组,支架置入前。B 组,成功置入支架后。箭头指示在其各自组中的狭窄点和支架放置感谢 Alvaro Alonso MD 和 Scott J. Gilbert MD 的支持 [Citation ends].
[Figure caption and citation for the preceding image starts]: 一位显著动脉粥样硬化性左肾动脉狭窄患者的数字减影血管造影。A 组,支架置入前。B 组,成功置入支架后。箭头指示在其各自组中的狭窄点和支架放置感谢 Alvaro Alonso MD 和 Scott J. Gilbert MD 的支持 [Citation ends]. [Figure caption and citation for the preceding image starts]: 左肾动脉的颜色和多普勒频谱显示湍流造成的颜色干扰,并且近端左肾动脉狭窄段流速增至 50 m/s,这符合显著肾动脉狭窄的特征感谢马萨诸塞大学纪念医疗保健血管实验室的注册医疗诊断超声医师 (RDMS) 兼注册血管技师 (RVT) Denise Kush 的支持 [Citation ends].虽然超声检查提供了一种安全的、非侵入性的评估手段,但其敏感性和特异性低,且使用这种检查仅提供了证明狭窄存在的间接证据。其他的非侵入性技术(即,CT 血管造影或磁共振血管造影)存在使用造影剂方面的风险(分别是造影剂肾病及肾源性系统性纤维化)。传统的血管造影尽管存在手术风险(例如,动脉粥样硬化性栓塞、出血)和造影剂肾病的风险,但可以测量狭窄病变部位的压力梯度,以及同时进行血管内治疗,具有能够确定病变临床意义的优势。
[Figure caption and citation for the preceding image starts]: 左肾动脉的颜色和多普勒频谱显示湍流造成的颜色干扰,并且近端左肾动脉狭窄段流速增至 50 m/s,这符合显著肾动脉狭窄的特征感谢马萨诸塞大学纪念医疗保健血管实验室的注册医疗诊断超声医师 (RDMS) 兼注册血管技师 (RVT) Denise Kush 的支持 [Citation ends].虽然超声检查提供了一种安全的、非侵入性的评估手段,但其敏感性和特异性低,且使用这种检查仅提供了证明狭窄存在的间接证据。其他的非侵入性技术(即,CT 血管造影或磁共振血管造影)存在使用造影剂方面的风险(分别是造影剂肾病及肾源性系统性纤维化)。传统的血管造影尽管存在手术风险(例如,动脉粥样硬化性栓塞、出血)和造影剂肾病的风险,但可以测量狭窄病变部位的压力梯度,以及同时进行血管内治疗,具有能够确定病变临床意义的优势。
对于患 RAS 临床概率较高的患者建议以非侵入性影像学检查开始。
患者的患病风险由临床医生的怀疑指数决定,该指数基于患者的人口学统计(高血压发病的年龄不足 30 岁或超过 55 岁)、合并症 (PVD、CAD、CVA),以及临床状况(难治性高血压且服用多于 3 种降压药)得出。
如果非侵入性检查的结果无法确诊,并且患 RAS 的临床疑似度较高,则推荐进行侵入性检查。
非侵入性影像学检查
首先进行肾脏超声检查较为合理,然后根据机构/医生的偏好进行 CT、MR 血管造影或卡托普利肾扫描。一些中心的初步检查首选 CT 或 MR 血管造影,如果对 CT 或 MR 血管造影有禁忌症,则进行肾多普勒超声或卡托普利肾扫描。
多普勒超声(灵敏度 84% 至 98%,特异性 62% 至 99%)。可以识别肾脏大小的差异、肾血流速度和阻力指数。[4]Chonchol M, Linas S. Diagnosis and management of ischemic nephropathy. Clin J Am Soc Nephrol. 2006;1:172-181.http://cjasn.asnjournals.org/content/1/2/172.fullhttp://www.ncbi.nlm.nih.gov/pubmed/17699206?tool=bestpractice.com[14]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:1425-1443.http://circ.ahajournals.org/content/127/13/1425.longhttp://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com[17]Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002;13(suppl 3):S184-S186.http://jasn.asnjournals.org/content/13/suppl_3/S184.fullhttp://www.ncbi.nlm.nih.gov/pubmed/12466311?tool=bestpractice.com显著肾动脉狭窄的超声诊断标准:[18]Gerhard-Herman M, Gardin JM, Jaff M, et al. Guidelines for noninvasive vascular laboratory testing: a report from the American Society of Echocardiography and the Society for Vascular Medicine and Biology. Vasc Med. 2006;11:183-200.http://vmj.sagepub.com/content/11/3/183.longhttp://www.ncbi.nlm.nih.gov/pubmed/17288127?tool=bestpractice.com
钆增强磁共振血管成像(敏感性 90% 至 100%,特异性 76% 至 94%)。[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006;113:e463-e654.http://circ.ahajournals.org/content/113/11/e463.longhttp://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com[4]Chonchol M, Linas S. Diagnosis and management of ischemic nephropathy. Clin J Am Soc Nephrol. 2006;1:172-181.http://cjasn.asnjournals.org/content/1/2/172.fullhttp://www.ncbi.nlm.nih.gov/pubmed/17699206?tool=bestpractice.com[14]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:1425-1443.http://circ.ahajournals.org/content/127/13/1425.longhttp://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com[17]Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002;13(suppl 3):S184-S186.http://jasn.asnjournals.org/content/13/suppl_3/S184.fullhttp://www.ncbi.nlm.nih.gov/pubmed/12466311?tool=bestpractice.com
CT 血管造影术(敏感性 59% 至 96%,特异性 82% 至 99%)。[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006;113:e463-e654.http://circ.ahajournals.org/content/113/11/e463.longhttp://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com[4]Chonchol M, Linas S. Diagnosis and management of ischemic nephropathy. Clin J Am Soc Nephrol. 2006;1:172-181.http://cjasn.asnjournals.org/content/1/2/172.fullhttp://www.ncbi.nlm.nih.gov/pubmed/17699206?tool=bestpractice.com[17]Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002;13(suppl 3):S184-S186.http://jasn.asnjournals.org/content/13/suppl_3/S184.fullhttp://www.ncbi.nlm.nih.gov/pubmed/12466311?tool=bestpractice.com[19]Olbricht CJ, Paul K, Prokop M, et al. Minimally invasive diagnosis of renal artery stenosis by spiral computed tomography angiography. Kidney Int. 1995;48:1332-1337.http://www.ncbi.nlm.nih.gov/pubmed/8569096?tool=bestpractice.com
由于卡托普利肾扫描复杂性和较差的敏感性,且有更方便和更准确的检查方法可用,卡托普利肾扫描(敏感性 45% 至 94%,特异性 81% 至 100%)目前已不太重要。[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006;113:e463-e654.http://circ.ahajournals.org/content/113/11/e463.longhttp://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com[4]Chonchol M, Linas S. Diagnosis and management of ischemic nephropathy. Clin J Am Soc Nephrol. 2006;1:172-181.http://cjasn.asnjournals.org/content/1/2/172.fullhttp://www.ncbi.nlm.nih.gov/pubmed/17699206?tool=bestpractice.com[17]Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002;13(suppl 3):S184-S186.http://jasn.asnjournals.org/content/13/suppl_3/S184.fullhttp://www.ncbi.nlm.nih.gov/pubmed/12466311?tool=bestpractice.com美国心脏病学会基金会/美国心脏协会不推荐采用卡托普利肾扫描诊断 RAS。[14]Anderson JL, Halperin JL, Albert NM, et al. Management of patients with peripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline recommendations): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:1425-1443.http://circ.ahajournals.org/content/127/13/1425.longhttp://www.ncbi.nlm.nih.gov/pubmed/23457117?tool=bestpractice.com
侵入性检查
传统血管造影术:[2]Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 practice guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic). Circulation. 2006;113:e463-e654.http://circ.ahajournals.org/content/113/11/e463.longhttp://www.ncbi.nlm.nih.gov/pubmed/16549646?tool=bestpractice.com[4]Chonchol M, Linas S. Diagnosis and management of ischemic nephropathy. Clin J Am Soc Nephrol. 2006;1:172-181.http://cjasn.asnjournals.org/content/1/2/172.fullhttp://www.ncbi.nlm.nih.gov/pubmed/17699206?tool=bestpractice.com[17]Zucchelli PC. Hypertension and atherosclerotic renal artery stenosis: diagnostic approach. J Am Soc Nephrol. 2002;13(suppl 3):S184-S186.http://jasn.asnjournals.org/content/13/suppl_3/S184.fullhttp://www.ncbi.nlm.nih.gov/pubmed/12466311?tool=bestpractice.com
