不明原因的头部外伤,颅骨骨折、硬膜下出血,通常合并颅脑外伤的临床体征和视网膜出血和/或视网膜剥脱(视网膜层裂),在没有任何潜在的代谢性疾病或临床显著出血性疾病或感染的情况下,高度提示虐待性头部外伤。
医院社区工作组及儿童保护组织在出现以上情况下应马上介入。 医疗评估可涉及受到案例法律方面影响的试验,如成骨不全症、先天性凝血异常或戊二酸尿 I 型试验。[29]Hartley LM, Khwaja OS, Verity CM. Glutaric aciduria type 1 and nonaccidental head injury. Pediatrics. 2001 Jan;107(1):174-5.http://www.ncbi.nlm.nih.gov/pubmed/11134453?tool=bestpractice.com
病史
在虐待性颅脑外伤时,照护者提供的病史通常与医学发现不一致。照护者可能诉无创伤史,或者提供并不足以导致头皮或颅骨损伤或者所见脑损伤程度的轻微创伤史。[2]Duhaime AC, Christian CW, Rorke LB, et al. Nonaccidental head injury in infants - the "shaken-baby syndrome." N Engl J Med. 1998 Jun 18;338(25):1822-9.http://www.ncbi.nlm.nih.gov/pubmed/9632450?tool=bestpractice.com[30]Piteau SJ, Ward MG, Barrowman NJ, et al. Clinical and radiographic characteristics associated with abusive and nonabusive head trauma: a systematic review. Pediatrics. 2012 Aug;130(2):315-23.http://pediatrics.aappublications.org/content/130/2/315.longhttp://www.ncbi.nlm.nih.gov/pubmed/22778309?tool=bestpractice.com 很显然,施暴者与患儿有一段独处的时间,并且他们会说是孩子能力发育不足引起的(比如说一个2月大婴儿自行爬行至床边摔下来)。当施暴者面对不同医师询问时通常给出不同的受伤过程。这也会延误治疗过程,一个伤害婴儿者通常会通知其正在工作的父母,在急救人员到来之前会采取措施让患儿醒来。一项对施暴者口供的研究发现,91%的被摇晃患儿会立即出现窒息、惊厥、呕吐、肌肉张力下降等症状。[15]Starling SP, Patel S, Burke BL, et al. Analysis of perpetrator admissions to inflicted traumatic brain injury in children. Arch Pediatr Adolesc Med. 2004 May;158(5):454-8.http://archpedi.ama-assn.org/cgi/content/full/158/5/454http://www.ncbi.nlm.nih.gov/pubmed/15123478?tool=bestpractice.com 如果儿童多次出现危及生命的事件,且仅在一名父母或看护者在场时发生及尚未发现其他医学解释时,可能需要进一步怀疑儿童虐待。[31]National Institute for Health and Care Excellence. Child maltreatment: when to suspect maltreatment in under 18s. October 2017 [internet publication].https://www.nice.org.uk/guidance/cg89
一些并发的疾病或近期接种疫苗导致的发热会增加诊断难度,比如患儿的烦躁或呕吐容易与病毒感染或脑膜炎混淆。 除此之外,症状会随着损伤程度有所改变,轻度损伤会出现渐进性症状。[1]Christian CW, Block R; Committee on Child Abuse and Neglect; American Academy of Pediatrics. Abusive head trauma in infants and children. Pediatrics. 2009 May;123(5):1409-11.http://pediatrics.aappublications.org/cgi/content/full/123/5/1409http://www.ncbi.nlm.nih.gov/pubmed/19403508?tool=bestpractice.com
很大一部分患儿都有外伤史或医学评估判定的外伤史。[32]Jenny C, Hymel KP, Ritzen A, et al. Analysis of missed cases of abusive head trauma. JAMA. 1999 Feb 17;281(7):621-6.http://www.ncbi.nlm.nih.gov/pubmed/10029123?tool=bestpractice.com 如果检查者不够细心,他们会将轻度损伤的症状误诊为胃肠炎、肠绞痛、脑膜炎或幽门狭窄。 放射科医师如果没接受儿科放射学培训会错过一些细微的对虐待性外伤具有诊断意义的发现。
一些轻伤患儿未被予以专业治疗而是让其自行恢复。 医师发现这些孩子会表现出头围增大。 非施暴父母可能完全不知道孩子已经受到了虐待。 婴儿可能因非相关的临床不适(如呼吸窘迫)被带来就医,并在做评估时意外发现人为伤害的体征,如胸片显示肋骨骨折。
各个经济水平的家庭都有可能发生虐待性头部外伤;然而,一项研究表明白人家庭已婚父母的孩子更容易被漏诊。[32]Jenny C, Hymel KP, Ritzen A, et al. Analysis of missed cases of abusive head trauma. JAMA. 1999 Feb 17;281(7):621-6.http://www.ncbi.nlm.nih.gov/pubmed/10029123?tool=bestpractice.com
病史中可能提示儿童虐待的其他要点包括其他已知危险因素,例如父母/照护者吸毒或酗酒、父母或照护者有心理健康问题,以及家庭成员有暴力侵犯史或既往儿童虐待史。[31]National Institute for Health and Care Excellence. Child maltreatment: when to suspect maltreatment in under 18s. October 2017 [internet publication].https://www.nice.org.uk/guidance/cg89
体格检查
体格检查通常不能发现损伤的外在体征。[1]Christian CW, Block R; Committee on Child Abuse and Neglect; American Academy of Pediatrics. Abusive head trauma in infants and children. Pediatrics. 2009 May;123(5):1409-11.http://pediatrics.aappublications.org/cgi/content/full/123/5/1409http://www.ncbi.nlm.nih.gov/pubmed/19403508?tool=bestpractice.com 囟门饱满或紧张,头围可能出现可记录的改变。 舌损伤不常见,但是黏膜损伤或唇、舌系带撕裂多见。 视网膜出血早期即可见,但通常是在行扩大的视网膜检查之后被发现。[30]Piteau SJ, Ward MG, Barrowman NJ, et al. Clinical and radiographic characteristics associated with abusive and nonabusive head trauma: a systematic review. Pediatrics. 2012 Aug;130(2):315-23.http://pediatrics.aappublications.org/content/130/2/315.longhttp://www.ncbi.nlm.nih.gov/pubmed/22778309?tool=bestpractice.com[33]Levin AV. Ophthalmology of shaken baby syndrome. Neurosurg Clin N Am. 2002 Apr;13(2):201-11, vi.http://www.ncbi.nlm.nih.gov/pubmed/12391704?tool=bestpractice.com 体检可发现虐待性长骨骨折;然而,许多骨折,例如后肋骨骨折和经典的干骺端病变(角骨折)通常没有表面淤血或肿胀。[30]Piteau SJ, Ward MG, Barrowman NJ, et al. Clinical and radiographic characteristics associated with abusive and nonabusive head trauma: a systematic review. Pediatrics. 2012 Aug;130(2):315-23.http://pediatrics.aappublications.org/content/130/2/315.longhttp://www.ncbi.nlm.nih.gov/pubmed/22778309?tool=bestpractice.com 包括咬伤或擦伤在内的皮肤表现可被发现;在不能行走的婴幼儿中任何擦伤等伤害都应提高关注度。[34]Nimkin K, Kleinman PK. Imaging of child abuse. Pediatr Clin North Am. 1997 Jun;44(3):615-35.http://www.ncbi.nlm.nih.gov/pubmed/9168871?tool=bestpractice.com 神经系统表现根据损伤的程度不同而存在差异;然而,通常存在一些脑损伤的临床体征。神经系统体征可能包括:易激惹、呕吐、反射亢进或反射不对称、肌张力下降、癫痫发作或昏迷。存在不能适当解释的肛门生殖器症状或体征时,应提高对儿童虐待的关注。[31]National Institute for Health and Care Excellence. Child maltreatment: when to suspect maltreatment in under 18s. October 2017 [internet publication].https://www.nice.org.uk/guidance/cg89
儿科格拉斯哥昏迷量表包含 3 项评估:眼睛反应、语言反应、动作反应。最低可能值为 3(深度昏迷或死亡),而最高值为 15(完全清醒或意识清楚)。
最佳眼部反应(E):
无睁眼
疼痛刺激睁眼
语言吩咐睁眼
自发睁眼。
最佳语言反应(V):
无语言反应
婴儿痛苦时呻吟
婴儿疼痛时哭闹
婴儿烦躁不安且持续哭闹
幼儿咿呀作声(正常反应)。
最佳动作反应(M):
无动作反应
婴儿异常伸展(去脑状态)
婴儿异常屈曲(去皮质状态)
婴儿对疼痛刺激屈曲反应
婴儿对疼痛刺激定位反应
婴儿自发或有目的地动作。
在评估儿童头部外伤时,英国国家卫生与临床优化研究所 (National Institute of Health and Care Excellence, NICE) 建议采用格拉斯哥昏迷评分而非 AVPU(清醒、对声音、疼痛有反应、无反应)评分。[31]National Institute for Health and Care Excellence. Child maltreatment: when to suspect maltreatment in under 18s. October 2017 [internet publication].https://www.nice.org.uk/guidance/cg89 NICE 指出,在以下一种或者多种情况下,如果一名儿童在没有经确认的重大意外创伤或已知的医学病因时出现颅内损伤,则可能是儿童虐待:[31]National Institute for Health and Care Excellence. Child maltreatment: when to suspect maltreatment in under 18s. October 2017 [internet publication].https://www.nice.org.uk/guidance/cg89
视网膜检查
暴力性摇晃所致的虐待性头部外伤,视网膜、玻璃体出血以及外伤性视网膜剥离是这种外伤损伤的特点。[1]Christian CW, Block R; Committee on Child Abuse and Neglect; American Academy of Pediatrics. Abusive head trauma in infants and children. Pediatrics. 2009 May;123(5):1409-11.http://pediatrics.aappublications.org/cgi/content/full/123/5/1409http://www.ncbi.nlm.nih.gov/pubmed/19403508?tool=bestpractice.com[30]Piteau SJ, Ward MG, Barrowman NJ, et al. Clinical and radiographic characteristics associated with abusive and nonabusive head trauma: a systematic review. Pediatrics. 2012 Aug;130(2):315-23.http://pediatrics.aappublications.org/content/130/2/315.longhttp://www.ncbi.nlm.nih.gov/pubmed/22778309?tool=bestpractice.com[35]Maguire S, Pickerd N, Farewell D, et al. Which clinical features distinguish inflicted from non-inflicted brain injury? A systematic review. Arch Dis Child. 2009 Nov;94(11):860-7.http://adc.bmj.com/content/94/11/860.longhttp://www.ncbi.nlm.nih.gov/pubmed/19531526?tool=bestpractice.com[36]Levin AV. Retinal hemorrhage in abusive head trauma. Pediatrics. 2010 Nov;126(5):961-70.http://www.ncbi.nlm.nih.gov/pubmed/20921069?tool=bestpractice.com[37]Levin AV, Christian CW; Committee on Child Abuse and Neglect, Section on Ophthalmology. The eye examination in the evaluation of child abuse. Pediatrics. 2010 Aug;126(2):376-80.http://pediatrics.aappublications.org/content/126/2/376.longhttp://www.ncbi.nlm.nih.gov/pubmed/20660545?tool=bestpractice.com[38]Shein SL, Bell MJ, Kochanek PM, et al. Risk factors for mortality in children with abusive head trauma. J Pediatr. 2012 Oct;161(4):716-722.e1.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3437227/http://www.ncbi.nlm.nih.gov/pubmed/22578583?tool=bestpractice.com 视网膜出血也可见于颅骨挤压伤,但通常程度较轻。当患儿临床情况稳定时,应到眼科咨询,以进行扩瞳视网膜检查。如果患儿的临床情况尚处于危险期,可能需要推迟该检查。[21]Mungan NK. Update on shaken baby syndrome: ophthalmology. Curr Opin Ophthalmol. 2007 Sep;18(5):392-7.http://www.ncbi.nlm.nih.gov/pubmed/17700232?tool=bestpractice.com[33]Levin AV. Ophthalmology of shaken baby syndrome. Neurosurg Clin N Am. 2002 Apr;13(2):201-11, vi.http://www.ncbi.nlm.nih.gov/pubmed/12391704?tool=bestpractice.com[39]Levin A. Retinal hemorrhages: advances in understanding. Pediatr Clin North Am. 2009 Apr;56(2):333-44.http://www.ncbi.nlm.nih.gov/pubmed/19358919?tool=bestpractice.com
一般认为广泛的视网膜多层出血是与虐待性摇晃一同发生的,当与视网膜相连的玻璃体开始运动,对视网膜产生剪切力,并导致视网膜层的分离。 视网膜出血可为单侧或双侧出血。 然而,有 15-25% 的病例并无视网膜出血的证据。[33]Levin AV. Ophthalmology of shaken baby syndrome. Neurosurg Clin N Am. 2002 Apr;13(2):201-11, vi.http://www.ncbi.nlm.nih.gov/pubmed/12391704?tool=bestpractice.com[40]Watts P; Child Maltreatment Guideline Working Party of Royal College of Ophthalmologists UK. Abusive head trauma and the eye in infancy. Eye (Lond). 2013 Oct;27(10):1227-9.http://www.ncbi.nlm.nih.gov/pubmed/23989117?tool=bestpractice.com [Figure caption and citation for the preceding image starts]: 如图可见,虐待性头部外伤通常有视网膜广泛及多层出血来自医学博士 Alice Newton 的个人收集资料;经获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 如图可见,虐待性头部外伤通常有视网膜广泛及多层出血来自医学博士 Alice Newton 的个人收集资料;经获准使用 [Citation ends].
头颅影像学
明显怀疑有外伤性脑损伤的患儿,或是怀疑受到过更多虐待的患儿都需要进行头颅影像检查。[41]Laskey AL, Holsti M, Runyan DK, et al. Occult head trauma in young suspected victims of physical abuse. J Pediatr. 2004 Jun;144(6):719-22.http://www.ncbi.nlm.nih.gov/pubmed/15192615?tool=bestpractice.com[42]Kemp AM, Rajaram S, Mann M, et al; Welsh Child Protection Systematic Review Group. What neuroimaging should be performed in children in whom inflicted brain injury (iBI) is suspected? A systematic review. Clin Radiol. 2009 May;64(5):473-83.http://www.ncbi.nlm.nih.gov/pubmed/19348842?tool=bestpractice.com[43]American College of Radiology. ACR appropriateness criteria: suspected physical abuse - child. 2016 [internet publication].https://acsearch.acr.org/docs/69443/Narrative 对于<6 月龄的婴儿,如果发现有其他躯体虐待损伤,应总是进行头部影像学检查。为了对患儿进行诊断和治疗,也为了保护在发生虐待的同一环境中接受照料的其他儿童(例如兄弟姐妹),应尽快进行影像学检查。
考虑到速度与可用性,一般首先进行大脑 CT 扫描。 如果CT诊断出有人为性脑部外伤,或者CT结果显示阴性但仍然高度怀疑虐待性头部外伤时,应该进一步行MRI检查。[43]American College of Radiology. ACR appropriateness criteria: suspected physical abuse - child. 2016 [internet publication].https://acsearch.acr.org/docs/69443/Narrative患儿出现不明原因的头围增加或是病情非常不稳定时,头颅超声能帮助识别硬膜下出血,还能识别蛛网膜下腔积液或硬膜下积液。然而,头颅超声可能无法分辨出范围较小的硬膜下积液。
在英国,NICE 建议在发现多个危险因素(包括怀疑任何非意外损伤时)1 小时内进行 CT 扫描。[31]National Institute for Health and Care Excellence. Child maltreatment: when to suspect maltreatment in under 18s. October 2017 [internet publication].https://www.nice.org.uk/guidance/cg89 根据临床表现的不同,也可能需要进行颈椎 CT 扫描或脊柱 MRI 来排除脊柱损伤。
大多数人为脑损伤病例通常需要进行神经科咨询,特别是有颅内压增高症状或体征时,如易怒、呕吐和囟门紧张或有放射学证据。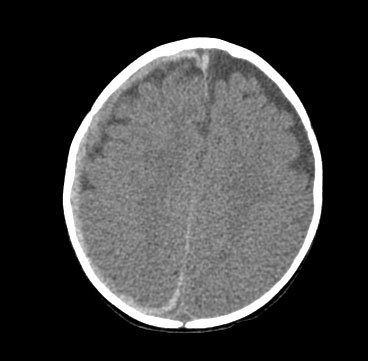 [Figure caption and citation for the preceding image starts]: CT可见硬膜下出血延伸至右侧凸面及纵裂区,同时轴外液体空间扩大来自医学博士 Alice Newton 的个人收集资料;经获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: CT可见硬膜下出血延伸至右侧凸面及纵裂区,同时轴外液体空间扩大来自医学博士 Alice Newton 的个人收集资料;经获准使用 [Citation ends]. [Figure caption and citation for the preceding image starts]: 致命的虐待性头部外伤CT结果常显示有明显的脑水肿及灰白质交界区缺失和脑室消失。 在这种情况下,硬膜下血液往往是难以发现来自医学博士 Alice Newton 的个人收集资料;经获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 致命的虐待性头部外伤CT结果常显示有明显的脑水肿及灰白质交界区缺失和脑室消失。 在这种情况下,硬膜下血液往往是难以发现来自医学博士 Alice Newton 的个人收集资料;经获准使用 [Citation ends]. [Figure caption and citation for the preceding image starts]: 虐待性头部外伤的MRI显示重度脑萎缩周围的硬膜下水囊瘤。 孩子最初被误诊为脑膜炎来自医学博士 Alice Newton 的个人收集资料;经获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 虐待性头部外伤的MRI显示重度脑萎缩周围的硬膜下水囊瘤。 孩子最初被误诊为脑膜炎来自医学博士 Alice Newton 的个人收集资料;经获准使用 [Citation ends].
骨骼影像学检查
如果怀疑<2 岁的儿童遭受过躯体虐待,则需要对其进行全身骨骼检查,对于经选择的≤3-4 岁的儿童,可能也需要进行该检查。如果条件允许,这项检查最好在有儿科放射科医生可读片的医疗中心进行。两周后的随访骨骼检查可能识别出最初检查没有看见的微小损伤或急性损伤。[34]Nimkin K, Kleinman PK. Imaging of child abuse. Pediatr Clin North Am. 1997 Jun;44(3):615-35.http://www.ncbi.nlm.nih.gov/pubmed/9168871?tool=bestpractice.com 如果骨骼检查后仍然留有不能解决的问题,那么可以采用骨闪烁扫描术作为有效的辅助检查方式。[34]Nimkin K, Kleinman PK. Imaging of child abuse. Pediatr Clin North Am. 1997 Jun;44(3):615-35.http://www.ncbi.nlm.nih.gov/pubmed/9168871?tool=bestpractice.com
其他检查
最初的实验室检查应包括全血细胞计数 (FBC)、血培养(如果有发热)、肝功能检查(用来评估腹部损伤)和凝血检查(包括凝血酶原时间、von Willebrand 试验和纤维蛋白原)。为了检查有无感染(如果出现发热)以及是否患 I 型戊二酸尿症,应进行尿液检查。尽管许多国家在新生儿筛查时检查此病,但初始检测可能呈阴性。戊二酸尿症一般有阳性家族史(常染色体隐性遗传)、小头畸形、运动迟缓和智力低下,但这些体征和症状可能未在年幼婴儿中表现出现来。[29]Hartley LM, Khwaja OS, Verity CM. Glutaric aciduria type 1 and nonaccidental head injury. Pediatrics. 2001 Jan;107(1):174-5.http://www.ncbi.nlm.nih.gov/pubmed/11134453?tool=bestpractice.com[44]Fernando S, Obaldo RE, Walsh IR, et al. Neuroimaging of nonaccidental head trauma: pitfalls and controversies. Pediatr Radiol. 2008 Aug;38(8):827-38.http://www.ncbi.nlm.nih.gov/pubmed/18176805?tool=bestpractice.com 所以最好还是做尿液毒理学检测以排除家中可能存在的违禁药物接触。
如果临床体征提示脑膜炎或脑炎,除非有禁忌证,否则应安排腰椎穿刺。在有创伤性脑损伤时,脑脊液检查显示大量红细胞而葡萄糖水平正常,如果损伤发生在就诊前至少 8-12 小时,则可能显示黄变症。[1]Christian CW, Block R; Committee on Child Abuse and Neglect; American Academy of Pediatrics. Abusive head trauma in infants and children. Pediatrics. 2009 May;123(5):1409-11.http://pediatrics.aappublications.org/cgi/content/full/123/5/1409http://www.ncbi.nlm.nih.gov/pubmed/19403508?tool=bestpractice.com
如果出现不明原因骨折,应检测血清 1,25-二羟基维生素 D、血钙、血磷和血镁水平,以排除诸如佝偻病等代谢性障碍疾病。即使无可疑的临床病史或体格检查结果,也需进行针对成骨不全症的检查。一般来说,这是通过检测血液中与成骨不全症有关的已知 DNA 突变来完成的,但是在经选择的病例中,也行皮肤活检(检测由成纤维细胞培养产生的胶原蛋白水平)。
鉴于虐待性外伤可能有法律后果(虽然机会不大),因此排除其他鉴别诊断是非常重要的。 遗传学医生和血液病医生的会诊具有指导意义。
任何不能解释的婴儿死亡必须做尸检以在确诊儿童猝死综合征之前明确是否有外伤、感染及其他医学方面的因素。
法律思考
当发现潜在的儿童虐待病例时,应尽快咨询医院儿童保护团队和社会工作服务机构,这是非常重要的。儿童保护服务机构将评估患儿和同一照护者所照顾的其他儿童再次受伤的风险。对家庭和其他照护者进行评估后,儿童保护服务机构可能会采取措施,避免儿童接触施加暴力的照护者。
此外,大多数人为头部外伤的案例将被转至警方或相关主管当局进行刑事调查。
