诊断通常是基于梗阻性脑积水体征和症状,在较少情况下,基于小脑功能障碍,大脑第四脑室存在造影增强肿块。[23]Kadin ME, Rubinstein LJ, Nelson JS. Neonatal cerebellar medulloblastoma originating from the fetal external granular layer. J Neuropathol Exp Neurol. 1970 Oct;29(4):583-600.http://www.ncbi.nlm.nih.gov/pubmed/5471923?tool=bestpractice.com[24]Raaf J, Kernohan JW. Relation of abnormal collections of cells in posterior medullary velum of cerebellum to origin of medulloblastoma. Arch Neurol. 1944 Sep;52(3):163-9.https://jamanetwork.com/journals/archneurpsyc/article-abstract/649950[25]Yachnis AT, Rorke LB, Trojanowski JQ. Cerebellar dysplasias in humans: development and possible relationship to glial and primitive neuroectodermal tumors of the cerebellar vermis. J Neuropathol Exp Neurol. 1994 Jan;53(1):61-71.http://www.ncbi.nlm.nih.gov/pubmed/8301321?tool=bestpractice.com[26]Packer RJ, Cogen P, Vezina G, et al. Medulloblastoma: clinical and biologic aspects. Neuro Oncol. 1999 Jul;1(3):232-50.http://www.ncbi.nlm.nih.gov/pubmed/11550316?tool=bestpractice.com[27]Roberts RO, Lynch CF, Jones MP, et al. Medulloblastoma: a population-based study of 532 cases. J Neuropathol Exp Neurol. 1991 Mar;50(2):134-44.http://www.ncbi.nlm.nih.gov/pubmed/2010773?tool=bestpractice.com[28]Giangaspero F, Perilongo G, Fondelli MP, et al. Medulloblastoma with extensive nodularity: a variant with favorable prognosis. J Neurosurg. 1999 Dec;91(6):971-7.http://www.ncbi.nlm.nih.gov/pubmed/10584843?tool=bestpractice.com[29]Pizer B, Clifford S. Medulloblastoma: new insights into biology and treatment. Arch Dis Child Educ Pract Ed. 2008 Oct;93(5):137-44.http://www.ncbi.nlm.nih.gov/pubmed/18809691?tool=bestpractice.com 可能在诊断前几周至几个月出现症状。
病史
极低龄儿童可能无法表达其感觉,所以通常是家长描述其儿童行为的改变(例如易激惹、社交互动下降)。 由肿瘤导致的梗阻性脑积水引起头痛、恶心和呕吐,就诊时有>80% 的患者可出现这些症状。 头痛和呕吐通常出现在早晨,并且在当天得到改善,虽然在当天任何时间都可能出现症状。 呕吐发生时不伴有发热或者感染的其他体征,通常可以缓解头痛。[22]Choux M, Lena G, Alfonsi S, et al. Medulloblastoma [in French]. Neurochirurgie. 1982;28 Suppl 1:1-229.http://www.ncbi.nlm.nih.gov/pubmed/7110502?tool=bestpractice.com 患者也可能主诉视觉障碍,最常见的是复视。 出现脊髓转移灶的病例可能表现出背痛、力弱和/或肠道或膀胱功能障碍。
体格检查
检查结果通常正常。 如果出现体征,通常与梗阻性脑积水有关(例如水平凝视受损或由于第六神经麻痹引起的复视、视盘水肿),而不是肿瘤本身(例如共济失调、眼球震颤、头部倾斜、辨距不良)。 小于18 个月的婴儿可能表现头围快速增加或前囟凸起。 仅表现颅神经病变的患者很少存在髓母细胞瘤,并且更可能存在脑干胶质瘤。
检查
脑部计算机体层成像 (CT) 和磁共振成像 (MRI) 作为第一步检测来确认初步诊断。CT 作为一种快速筛查的有效手段;但是 MRI 是进行肿瘤评估并进行有无脑或脊髓转移的诊断标准。较之于 MRI,CT 的优势是更快进行筛查,不需要镇静,并且更容易在紧急情况下进行。较之于 CT,MRI 的优势是可更好地观察大脑,并且不涉及放射性暴露。[30]Goldstein AM, Yuen J, Tucker MA. Second cancers after medulloblastoma: population-based results from the United States and Sweden. Cancer Causes Control. 1997 Nov;8(6):865-71.http://www.ncbi.nlm.nih.gov/pubmed/9427429?tool=bestpractice.com
应该在以下情况中对患者进行大脑 CT 或 MRI检查:[22]Choux M, Lena G, Alfonsi S, et al. Medulloblastoma [in French]. Neurochirurgie. 1982;28 Suppl 1:1-229.http://www.ncbi.nlm.nih.gov/pubmed/7110502?tool=bestpractice.com
对大脑和整个脊柱通过平扫和对比增强 MRI 进行仔细的转移评估是必须的。
从手术中恢复后,应该检查脑脊液 (CSF) 是否存在肿瘤细胞。 据证明,距手术至少 15 天后通过腰椎穿刺术采集的 CSF 比脑室 CSF 在进行肿瘤分期方面更可靠。[31]Gajjar A, Fouladi M, Walter AW, et al. Comparison of lumbar and shunt cerebrospinal fluid specimens for cytologic detection of leptomeningeal disease in pediatric patients with brain tumors. J Clin Oncol. 1999 Jun;17(6):1825-8.http://www.ncbi.nlm.nih.gov/pubmed/10561221?tool=bestpractice.com 所有患者均应该接受腰椎穿刺,无论患者处于哪一年龄段,也无论 MRI 有何种显示。
术后 MRI 对于切除范围的评估很重要,并且应该在肿瘤切除的 48 小时内进行,在该时间段之后,术后变化将使得解释残留病变变得困难。 如果在该时间窗内无法进行,则至少不要在术后 10 天内进行。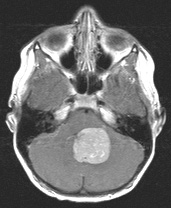 [Figure caption and citation for the preceding image starts]: MRI:髓母细胞瘤轴状位观图、采用钆增强 T1WI,显示明显强化的实质性和囊性病变填充第四脑室;资料由 Peter B. Storm 提供,获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: MRI:髓母细胞瘤轴状位观图、采用钆增强 T1WI,显示明显强化的实质性和囊性病变填充第四脑室;资料由 Peter B. Storm 提供,获准使用 [Citation ends].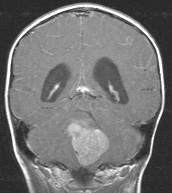 [Figure caption and citation for the preceding image starts]: MRI:髓母细胞瘤冠状位观图、采用钆增强的 T1WI,显示明显强化的实质性和囊性病变填充第四脑室;出现梗阻性脑积水。资料由 Peter B. Storm 提供,获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: MRI:髓母细胞瘤冠状位观图、采用钆增强的 T1WI,显示明显强化的实质性和囊性病变填充第四脑室;出现梗阻性脑积水。资料由 Peter B. Storm 提供,获准使用 [Citation ends]. [Figure caption and citation for the preceding image starts]: MRI:髓母细胞瘤的矢状位观图、采用钆增强的 T1WI、显示自患者的第四脑室后部髓母细胞瘤的多处显著增强的下行转移。资料由 Peter B. Storm 提供,获准使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: MRI:髓母细胞瘤的矢状位观图、采用钆增强的 T1WI、显示自患者的第四脑室后部髓母细胞瘤的多处显著增强的下行转移。资料由 Peter B. Storm 提供,获准使用 [Citation ends].
病理学
所有患者应该接受手术切除肿瘤,以获得诊断,并且根据组织学亚组结果得出预后情况。 根据病理学家对大体标本、显微镜发现和免疫组织化学染色结果的评估得出诊断。[3]Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016 May 9;131(6):803-20.https://link.springer.com/article/10.1007%2Fs00401-016-1545-1http://www.ncbi.nlm.nih.gov/pubmed/27157931?tool=bestpractice.com
