应对就诊时存在骨痛的所有患者考虑骨肉瘤的诊断,尤其是当患者年龄为十几岁到二十几岁时。 超过该年龄段的患者很少受影响,这些病例更多的是倾向于与先前的放疗或佩吉特病史相关的继发性骨肉瘤。 即使是最初的 X线平片不确定是否为骨肉瘤的情况下,都应将患者转诊至肿瘤科主任医生处进行相应处理。
临床发现
骨肉瘤具体的体检发现取决于肿瘤所在的位置。 疼痛、肿胀、跛行或关节活动度受限是最常见的症状,出现这类症状时应提高对骨肿瘤可能性的怀疑。[2]Canale, ST. Campbell's operative orthopedics. 10th ed. Philadelphia, USA: Mosby; 2003.[4]Campanacci M. Bone and soft tissue tumors: clinical features, imaging, pathology and treatment. 2nd ed. New York, NY: Springer; 1999. 受累区域可见局部肿胀伴相关性皮肤发热以及偶尔出现溃疡。患者很少会出现病理性骨折,病理性骨折在单纯的溶骨性肿瘤(例如,毛细血管扩张性骨肉瘤)中较常见。转移性肿瘤(主要是肺部)相关症状也是临床现象的一部分。
初始检查
2 个位面的常规 X 光平片检查是最可靠的骨肉瘤一线诊断方式。 这些 X 光平片上的典型表现为射线强度斑驳且边界不清的射线可透过的区域。 肿瘤通常位于长骨的干骺端。 骨膜下的反应性新骨形成会被看成 Codman 三角或者可以提供日光放射样的外表特征。 有时,常规 X 线片上也可以看到软组织肿块。[13]Letson D, Falcone R, Muro-Cacho C. Pathologic and radiologic features of primary bone tumors. Cancer Control. 1999 May;6(3):283-93.http://www.ncbi.nlm.nih.gov/pubmed/10758559?tool=bestpractice.com
骨肉瘤无特定的实验室检查:碱性磷酸酶和乳酸脱氢酶水平可能会升高,且可能会带来不良后果。[14]Casali PG, Bielack S, Abecassis N, et al. Bone sarcomas: ESMO-PaedCan-EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018 Oct 1;29(suppl 4):iv79-95.https://academic.oup.com/annonc/article/29/Supplement_4/iv79/5115250http://www.ncbi.nlm.nih.gov/pubmed/30285218?tool=bestpractice.com 通常,碱性磷酸酶的检测对监控治疗后复发更有效果。[2]Canale, ST. Campbell's operative orthopedics. 10th ed. Philadelphia, USA: Mosby; 2003.[4]Campanacci M. Bone and soft tissue tumors: clinical features, imaging, pathology and treatment. 2nd ed. New York, NY: Springer; 1999.[13]Letson D, Falcone R, Muro-Cacho C. Pathologic and radiologic features of primary bone tumors. Cancer Control. 1999 May;6(3):283-93.http://www.ncbi.nlm.nih.gov/pubmed/10758559?tool=bestpractice.com[15]Malawer MM, Sugarbaker PH. Musculoskeletal cancer surgery: treatment of sarcomas and allied diseases. Dordrecht: Kluwer Academic Publishers; 2001.http://www.sarcoma.org/Sarcoma/index.php?db=content/Sarcoma&tbl=Publications&id=8 如果 X 光平片检查结果为阴性,但症状仍然持续甚至更糟,则需要进行计算机体层成像扫描 (CT) 或磁共振成像 (MRI) 扫描。 [Figure caption and citation for the preceding image starts]: 常规 X 线平片,前后位;累及股骨远端干骺端的渗入性病变,边界不清,同时存在射线不透性和射线可透性外观;还存在一处较大的软组织肿块,伴有骨膜反应Dr Michael J. Klein 和 Dr Luminita Rezeanu 的个人收藏 [Citation ends].
[Figure caption and citation for the preceding image starts]: 常规 X 线平片,前后位;累及股骨远端干骺端的渗入性病变,边界不清,同时存在射线不透性和射线可透性外观;还存在一处较大的软组织肿块,伴有骨膜反应Dr Michael J. Klein 和 Dr Luminita Rezeanu 的个人收藏 [Citation ends].
局部分期
MRI 和 CT 用于确定局部分期时同样准确。在一项涉及 387 例骨肉瘤和尤文氏肉瘤患者的研究中,MRI 和 CT 在确定局部肿瘤范围时没有显著的统计学差异。[16]Meyer JS, Nadel HR, Marina N, et al. Imaging guidelines for children with Ewing sarcoma and osteosarcoma: a report from the Children's Oncology Group Bone Tumor Committee. Pediatr Blood Cancer. 2008 Aug;51(2):163-70.http://www.ncbi.nlm.nih.gov/pubmed/18454470?tool=bestpractice.com 但 MRI 通常因其对软组织对比有较高的敏感性、多平面能力以及无辐射接触而更受欢迎。 此外,MRI 还可以评估生长板穿孔、关节间隙浸润、肿瘤是否可包覆并使神经血管束移位,以及是否存在相邻肌肉的浸润。 因此,用 MRI 评估的区域应该包括整个受累骨段及相邻的关节。[14]Casali PG, Bielack S, Abecassis N, et al. Bone sarcomas: ESMO-PaedCan-EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018 Oct 1;29(suppl 4):iv79-95.https://academic.oup.com/annonc/article/29/Supplement_4/iv79/5115250http://www.ncbi.nlm.nih.gov/pubmed/30285218?tool=bestpractice.com CT 可用于显示肿瘤生成的少量基质及不正常位置的骨膜反应,并且其在检测肺部是否存在转移方面也明显优于常规 X 线平片。[16]Meyer JS, Nadel HR, Marina N, et al. Imaging guidelines for children with Ewing sarcoma and osteosarcoma: a report from the Children's Oncology Group Bone Tumor Committee. Pediatr Blood Cancer. 2008 Aug;51(2):163-70.http://www.ncbi.nlm.nih.gov/pubmed/18454470?tool=bestpractice.com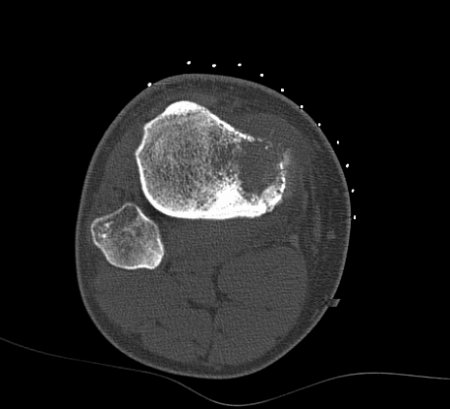 [Figure caption and citation for the preceding image starts]: 计算机断层 (CT) 扫描,轴位;胫骨近端骨肉瘤;基质生成和骨破坏可以在传统断层 X 光摄影装置上得到最佳呈现。Dr Michael J. Klein 和 Dr Luminita Rezeanu 的个人收藏 [Citation ends].
[Figure caption and citation for the preceding image starts]: 计算机断层 (CT) 扫描,轴位;胫骨近端骨肉瘤;基质生成和骨破坏可以在传统断层 X 光摄影装置上得到最佳呈现。Dr Michael J. Klein 和 Dr Luminita Rezeanu 的个人收藏 [Citation ends].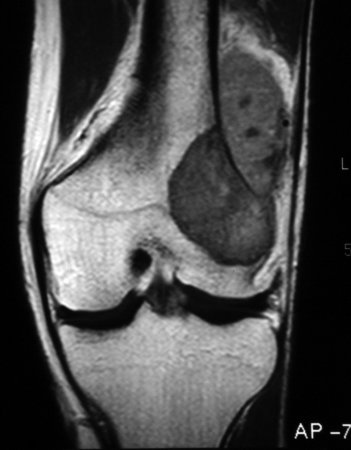 [Figure caption and citation for the preceding image starts]: 磁共振成像,冠状位;股骨远端骨肉瘤显示低密度信号;T1 加权成像;实际骨内和骨外肿瘤范围也能看到Dr Michael J. Klein 和 Dr Luminita Rezeanu 的个人收藏 [Citation ends].
[Figure caption and citation for the preceding image starts]: 磁共振成像,冠状位;股骨远端骨肉瘤显示低密度信号;T1 加权成像;实际骨内和骨外肿瘤范围也能看到Dr Michael J. Klein 和 Dr Luminita Rezeanu 的个人收藏 [Citation ends].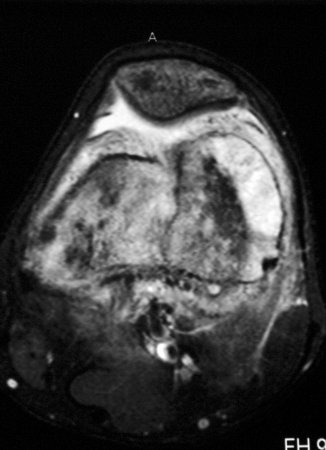 [Figure caption and citation for the preceding image starts]: 磁共振成像,轴位;股骨远端骨肉瘤显示高密度信号;T2 加权成像Dr Michael J. Klein 和 Dr Luminita Rezeanu 的个人收藏 [Citation ends].
[Figure caption and citation for the preceding image starts]: 磁共振成像,轴位;股骨远端骨肉瘤显示高密度信号;T2 加权成像Dr Michael J. Klein 和 Dr Luminita Rezeanu 的个人收藏 [Citation ends].
活组织检查
肿瘤的组织学检查是确定性诊断检查。 空芯针活检或开放性活检是推荐的活检技术。[17]National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: bone cancer [internet publication].http://www.nccn.org/professionals/physician_gls/f_guidelines.asp 活检应在专门从事骨肉瘤治疗的中心进行,且只能在已使用常规 X 线平片、CT 和 MRI 完成局部分期后进行。 不建议进行细针抽吸活检和切除活检。 应尽快提交肿瘤组织进行病理评估。 可获取肿瘤印片(术中细胞学印片),并应将组织速冻和/或送至细胞遗传学分析。 肿瘤库对于癌症的诊断以及分子病理学的转化研究都非常有用;因此,应根据当地实际情况寻求肿瘤库的知情同意书以便日后分析和研究。[14]Casali PG, Bielack S, Abecassis N, et al. Bone sarcomas: ESMO-PaedCan-EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018 Oct 1;29(suppl 4):iv79-95.https://academic.oup.com/annonc/article/29/Supplement_4/iv79/5115250http://www.ncbi.nlm.nih.gov/pubmed/30285218?tool=bestpractice.com 为最大程度降低误诊可能性和优化诊疗结果,任何骨肿瘤都应由矫形外科肿瘤学专家进行评估。 活检和后期切除术最好由同一位临床医生进行。[15]Malawer MM, Sugarbaker PH. Musculoskeletal cancer surgery: treatment of sarcomas and allied diseases. Dordrecht: Kluwer Academic Publishers; 2001.http://www.sarcoma.org/Sarcoma/index.php?db=content/Sarcoma&tbl=Publications&id=8 为降低活检过程中引起播种肿瘤的风险,活检针道或瘢痕应在后期切除术中予以去除。
系统性分期与病情检查
确诊后的系统性分期重点关注转移的主要部位:肺部以及骨骼。各类检查包括胸部 X 线平片检查、高分辨率肺部和胸部螺旋 CT 扫描,以及用于检测跳跃性病变和远处转移的放射性核素骨扫描。数据表明,在骨肉瘤患者的初步评估中,18 氟-氟代脱氧葡萄糖正电子发射断层扫描 CT 也可能有价值,可以代替放射性核素骨扫描,也可以作为辅助手段。[18]Hurley C, McCarville MB, Shulkin BL, et al. Comparison of (18) F-FDG-PET-CT and bone scintigraphy for evaluation of osseous metastases in newly diagnosed and recurrent osteosarcoma. Pediatr Blood Cancer. 2016 Aug;63(8):1381-6.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5082741/http://www.ncbi.nlm.nih.gov/pubmed/27082077?tool=bestpractice.com 这些检查可由受累部位的 X 线平片和/或 MRI 进行补充。手术前必须反复对原发性肿瘤或已知转移部位进行恰当的影像学检查。[14]Casali PG, Bielack S, Abecassis N, et al. Bone sarcomas: ESMO-PaedCan-EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018 Oct 1;29(suppl 4):iv79-95.https://academic.oup.com/annonc/article/29/Supplement_4/iv79/5115250http://www.ncbi.nlm.nih.gov/pubmed/30285218?tool=bestpractice.com
治疗前可进行其他与病情相关的实验室检查,包括全血细胞计数和分类计数、血型分型、凝血功能检查、血清电解质(包括镁和磷酸盐)检查、肝肾功能检查,以及肝炎和 HIV 的检查。
由于骨肉瘤的化疗治疗会导致心功能障碍和听觉障碍,可通过超声心动图或放射性核素腔室造影联合听力图对心功能及听力进行基线评估。 建议对生育年龄的男性的精液进行储存。[14]Casali PG, Bielack S, Abecassis N, et al. Bone sarcomas: ESMO-PaedCan-EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018 Oct 1;29(suppl 4):iv79-95.https://academic.oup.com/annonc/article/29/Supplement_4/iv79/5115250http://www.ncbi.nlm.nih.gov/pubmed/30285218?tool=bestpractice.com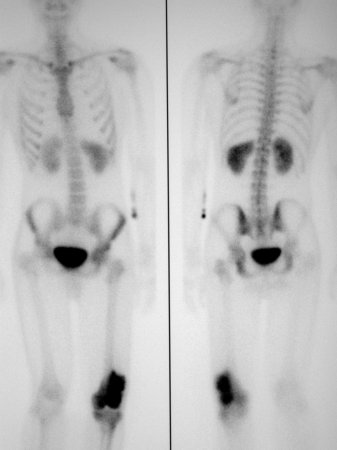 [Figure caption and citation for the preceding image starts]: 骨扫描;肿瘤部位放射性核素吸收较高Dr Michael J. Klein 和 Dr Luminita Rezeanu 的个人收藏 [Citation ends].
[Figure caption and citation for the preceding image starts]: 骨扫描;肿瘤部位放射性核素吸收较高Dr Michael J. Klein 和 Dr Luminita Rezeanu 的个人收藏 [Citation ends].
