对于表现出轻微临床症状的免疫力正常的人群,组织胞浆菌病的诊断可根据流行地区旅游史和流感样症状诊断。
对于免疫力缺陷或表现出持续呼吸道症状的患者,须完整采集病史,体格检查,并根据临床,影像学,实验室检查评估是否存在疾病播散。
病史
应获得完整的职业史和社交史。组织胞浆菌病流行于美国的俄亥俄州,密西西比,密苏里河流域,和中南美洲地区。[3]Cano MV, Hajjeh RA. The epidemiology of histoplasmosis: a review. Semin Respir Infect. 2001;16:109-118.http://www.ncbi.nlm.nih.gov/pubmed/11521243?tool=bestpractice.com[4]Mata-Essayag S, Colella MT, Rosello A, et al. Histoplasmosis: a study of 158 cases in Venezuela, 2000-2005. Medicine (Baltimore). 2008;87:193-202.http://www.ncbi.nlm.nih.gov/pubmed/18626302?tool=bestpractice.com可能感染肺组织胞浆菌病的活动包括:洞穴探险,接触鸡舍,挖据拆迁活动或伐木。询问相关病史有助于明确真菌孢子暴露量的评估。
患者可能有相关用药史或其它共存疾病导致的免疫缺陷。
患者可能患有基础肺部疾病(如肺气肿)。慢性肺病是发生慢性肺组织胞浆菌病的危险因素。[20]Wheat LJ, Wass J, Norton J, et al. Cavitary histoplasmosis occurring during two large urban outbreaks. Analysis of clinical, epidemiologic, roentgenographic, and laboratory features. Medicine (Baltimore). 1984;63:201-209.http://www.ncbi.nlm.nih.gov/pubmed/6738342?tool=bestpractice.com[21]Wheat LJ, Conces D, Allen SD, et al. Pulmonary histoplasmosis syndromes: recognition, diagnosis, and management. Semin Respir Crit Care Med. 2004;25:129-144.http://www.ncbi.nlm.nih.gov/pubmed/16088457?tool=bestpractice.com
因为其高发病率和高死亡率,在免疫缺陷(如HIV感染/艾滋病,使用TNF-alpha 拮抗剂或激素等免疫抑制剂),中性粒细胞减少症,<2岁,慢性肺病,接受干细胞或器官移植的患者中,在疾病早期应考虑到播散性真菌感染的可能。[14]Schwartz RS, Mackintosh FR, Schrier SL, et al. Multivariate analysis of factors associated with invasive fungal disease during remission induction therapy for acute myelogenous leukemia. Cancer. 1984;53:411-419.http://www.ncbi.nlm.nih.gov/pubmed/6581852?tool=bestpractice.com[15]Assi M, Martin S, Wheat LJ, et al. Histoplasmosis after solid organ transplant. Clin Infect Dis. 2013;57:1542-1549.http://www.ncbi.nlm.nih.gov/pubmed/24046304?tool=bestpractice.com[16]Kauffman CA, Freifeld AG, Andes DR, et al. Endemic fungal infections in solid organ and hematopoietic cell transplant recipients enrolled in the Transplant-Associated Infection Surveillance Network (TRANSNET). Transpl Infect Dis. 2014;16:213-224.http://www.ncbi.nlm.nih.gov/pubmed/24589027?tool=bestpractice.com
体格检查
无症状肺组织胞浆菌病
急性肺组织胞浆菌病(症状<4周)
患者可有流感样症状(如发热,头痛,乏力,腹痛,体重减轻,干咳,胸痛,关节疼痛等不适)。[1]Wheat LJ, Freifeld AG, Kleiman MB, et al. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis. 2007;45:807-825.http://cid.oxfordjournals.org/content/45/7/807.fullhttp://www.ncbi.nlm.nih.gov/pubmed/17806045?tool=bestpractice.com
查体常无明显异常。胸部听诊可正常,部分患者可听见散在罗音或支气管呼吸音。
急性肺组织胞浆菌病(症状>4周)
慢性肺组织胞浆菌病
播散型组织胞浆菌病
主要发生在免疫功能受损患者中,尤其是 HIV 感染患者中。[1]Wheat LJ, Freifeld AG, Kleiman MB, et al. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis. 2007;45:807-825.http://cid.oxfordjournals.org/content/45/7/807.fullhttp://www.ncbi.nlm.nih.gov/pubmed/17806045?tool=bestpractice.com
原发性免疫缺陷或由于使用TNF-alpha拮抗剂或免疫抑制剂等治疗引起的继发性免疫缺陷可以增加进行性,播散型组织胞浆菌病的风险,严重者可威胁生命。[11]Deepe GS Jr. Modulation of infection with Histoplasma capsulatum by inhibition of tumor necrosis factor-alpha activity. Clin Infect Dis. 2005;41(suppl 3):S204-S207.http://cid.oxfordjournals.org/content/41/Supplement_3/S204.fullhttp://www.ncbi.nlm.nih.gov/pubmed/15983901?tool=bestpractice.com[13]Wallis RS, Broder M, Wong J, et al. Reactivation of latent granulomatous infections by infliximab. Clin Infect Dis. 2005;41(suppl 3):S194-S198.http://cid.oxfordjournals.org/content/41/Supplement_3/S194.longhttp://www.ncbi.nlm.nih.gov/pubmed/15983899?tool=bestpractice.com
最常见的临床表现为发热;其它常见症状包括头痛,纳差,体重减轻,萎靡。
肺外表现因人而异,包括皮疹,肝脾肿大,肝酶升高,全血细胞减少,胃肠道反应,类败血症表现。[2]Wheat LJ, Connolly-Stringfield PA, Baker RL, et al. Disseminated histoplasmosis in the acquired immune deficiency syndrome: clinical findings, diagnosis and treatment, and review of the literature. Medicine (Baltimore). 1990;69:361-374.http://www.ncbi.nlm.nih.gov/pubmed/2233233?tool=bestpractice.com
中枢播散可表现为颅内病灶或脑膜炎。
在HIV感染者或艾滋病患者中,肺组织胞浆菌病常播散至全身,而肺部感染症状也较其它患者更为严重。
检查
胸片
所有患者应进行胸片检查。在轻症患者中,胸片可以评估肺部病情的程度,并能区别流感和社区获得性肺炎。
胸片中可见钙化肉芽肿,这些肉芽肿提示既往真菌感染或愈合的病灶。
胸片中可见到单侧或双侧间质性或网状性炎症浸润,结节,纵膈或胸门淋巴结肿大,空洞,胸腔积液等表现。
HIV感染者或免疫缺陷人群感染肺组织胞浆菌病时,可表现为双肺弥漫性网结节性的炎症浸润,与肺孢子菌肺炎的表现十分类似。[2]Wheat LJ, Connolly-Stringfield PA, Baker RL, et al. Disseminated histoplasmosis in the acquired immune deficiency syndrome: clinical findings, diagnosis and treatment, and review of the literature. Medicine (Baltimore). 1990;69:361-374.http://www.ncbi.nlm.nih.gov/pubmed/2233233?tool=bestpractice.com胸片上看到双侧弥漫性间质性肺炎应警惕播散型组织胞浆菌病的可能。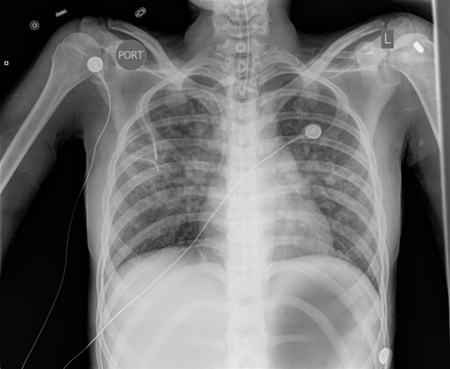 [Figure caption and citation for the preceding image starts]: 组织胞浆菌病患者的胸片,可见双侧弥漫性网状性浸润。资料来源于 David L. Goldman 医生的个人收集 [Citation ends].
[Figure caption and citation for the preceding image starts]: 组织胞浆菌病患者的胸片,可见双侧弥漫性网状性浸润。资料来源于 David L. Goldman 医生的个人收集 [Citation ends].
CT检查
当与临床表现和影像学检查结果相符时,实验室检查可作为诊断的基础。应认识到每一项实验室检查均有它的局限性。可从痰液,血液,尿液,支气管肺泡灌洗液或脑脊液中提取标本。通常,痰液,血液,尿液被用来进行检测,但如果病情较重而初步的诊断模棱两可,可提取支气管肺泡灌洗液或脑脊液进行进一步检测分析。
培养
在慢性肺组织胞浆菌病中或播散型组织胞浆菌病患者中,这一实验室检查最有意义。急性弥漫性肺炎和播散性组织胞浆菌病的患者菌量负荷高,因此,痰培养的阳性率可达到60-80%。[22]Wheat LJ. Improvements in diagnosis of histoplasmosis. Expert Opin Biol Ther. 2006;6:1207-1221.http://www.ncbi.nlm.nih.gov/pubmed/17049017?tool=bestpractice.com[23]Wheat LJ, Garringer T, Brizendine E, et al. Diagnosis of histoplasmosis by antigen detection based upon experience at the histoplasmosis reference laboratory. Diagn Microbiol Infect Dis. 2002;43:29-37.http://www.ncbi.nlm.nih.gov/pubmed/12052626?tool=bestpractice.com相反,急性局限性肺部感染的患者的真菌负荷量较低,因此,痰培养的敏感性只有15%。
组织胞浆菌生长较慢,需4-6周时间。样本可来自于痰液或支气管肺泡灌洗液。 [Figure caption and citation for the preceding image starts]: 在两个不同的琼脂上斜面培养荚膜组织胞浆菌。Lenore Haley 医生,美国疾病预防控制中心公共健康图片库 [Citation ends].
[Figure caption and citation for the preceding image starts]: 在两个不同的琼脂上斜面培养荚膜组织胞浆菌。Lenore Haley 医生,美国疾病预防控制中心公共健康图片库 [Citation ends].
支气管肺泡灌洗液培养在艾滋病患者中的敏感性为89%。[24]Wheat LJ, Connolly-Stringfield P, Williams B, et al. Diagnosis of histoplasmosis in patients with the acquired immunodeficiency syndrome by detection of Histoplasma capsulatum polysaccharide antigen in bronchoalveolar lavage fluid. Am Rev Respir Dis. 1992;145:1421-1424.http://www.ncbi.nlm.nih.gov/pubmed/1596012?tool=bestpractice.com
血清学(抗原检测):酶联免疫法(enzyme immunoassay, EIA)
该检测能够提供快速诊断,是基于荚膜组织胞浆菌半乳甘露聚糖的检测。它对重病患者很有帮助。样本可采用血清,尿液,支气管肺泡灌洗液,脑脊液。
急性弥漫性肺炎和播散性组织胞浆菌病的患者菌量负荷高,因此,尿抗原检测的阳性率可达到75%。[22]Wheat LJ. Improvements in diagnosis of histoplasmosis. Expert Opin Biol Ther. 2006;6:1207-1221.http://www.ncbi.nlm.nih.gov/pubmed/17049017?tool=bestpractice.com[23]Wheat LJ, Garringer T, Brizendine E, et al. Diagnosis of histoplasmosis by antigen detection based upon experience at the histoplasmosis reference laboratory. Diagn Microbiol Infect Dis. 2002;43:29-37.http://www.ncbi.nlm.nih.gov/pubmed/12052626?tool=bestpractice.com相反,急性局限性肺部感染的患者的菌量负荷较低,尿液中抗原检测的阳性率为大约30%。[25]Williams B, Fojtasek M, Connolly-Stringfield P, et al. Diagnosis of histoplasmosis by antigen detection during an outbreak in Indianapolis, Ind. Arch Pathol Lab Med. 1994;118:1205-1208.http://www.ncbi.nlm.nih.gov/pubmed/7979915?tool=bestpractice.com
尿抗原检测的敏感性相似或优于血清抗原检测。[26]Fandiño-Devia E, Rodríguez-Echeverri C, Cardona-Arias J, et al. Antigen detection in the diagnosis of histoplasmosis: a meta-analysis of diagnostic performance. Mycopathologia. 2016;181:197-205.http://www.ncbi.nlm.nih.gov/pubmed/26559429?tool=bestpractice.com它对诊断免疫功能受损的患者或重病且可能无法产生抗体应答的患者特别有帮助。[25]Williams B, Fojtasek M, Connolly-Stringfield P, et al. Diagnosis of histoplasmosis by antigen detection during an outbreak in Indianapolis, Ind. Arch Pathol Lab Med. 1994;118:1205-1208.http://www.ncbi.nlm.nih.gov/pubmed/7979915?tool=bestpractice.com
它对支气管肺泡灌洗液有85%的敏感性和92%特异性。[27]Hage CA, Davis TE, Egan L, et al. Diagnosis of pulmonary histoplasmosis and blastomycosis by detection of antigen in bronchoalveolar lavage fluid using an improved second-generation enzyme-linked immunoassay. Respir Med. 2007;101:43-47.http://www.ncbi.nlm.nih.gov/pubmed/16753290?tool=bestpractice.com
血清抗原含量会在治疗开始的两个星期里减少,而在尿液中的抗原含量会持续数月保持在低浓度随后逐渐消失。[28]Fojtasek MF, Kleiman MB, Connolly-Stringfield P, et al. The Histoplasma capsulatum antigen assay in disseminated histoplasmosis in children. Pediatr Infect Dis J. 1994;13:801-805.http://www.ncbi.nlm.nih.gov/pubmed/7808850?tool=bestpractice.com
对于播散性组织胞浆菌病患者或艾滋病患者,支气管肺泡灌洗液中抗原检测的敏感性与血清学检测相当。[24]Wheat LJ, Connolly-Stringfield P, Williams B, et al. Diagnosis of histoplasmosis in patients with the acquired immunodeficiency syndrome by detection of Histoplasma capsulatum polysaccharide antigen in bronchoalveolar lavage fluid. Am Rev Respir Dis. 1992;145:1421-1424.http://www.ncbi.nlm.nih.gov/pubmed/1596012?tool=bestpractice.com
血清学(抗体检测):免疫扩散沉淀试验
该检测在有症状的急性肺组织胞浆菌病的患者中的阳性率为90%,在慢性肺组织胞浆菌病的患者中的阳性率接近100%。该项检测敏感性较高,但由于交叉反应存在一些限制。
另外,抗体可在急性感染后4-8周内被检测到,并持续存在12-18个月。这可以解释为什么初期血清学检测可以为阴性,而在一个月后转阳。
流行地区的背景血清学阳性率较低,因此,免疫扩散试验在流行地区也有较高的敏感性。[29]Wheat J, French ML, Kohler RB, et al. The diagnostic laboratory tests for histoplasmosis: analysis of experience in a large urban outbreak. Ann Intern Med. 1982;97:680-685.http://www.ncbi.nlm.nih.gov/pubmed/6814316?tool=bestpractice.com
血清学抗体检测的报告可表现为:M或H条带可见。[22]Wheat LJ. Improvements in diagnosis of histoplasmosis. Expert Opin Biol Ther. 2006;6:1207-1221.http://www.ncbi.nlm.nih.gov/pubmed/17049017?tool=bestpractice.comH和M抗原是真菌释放的糖蛋白。M条带在急性肺组织胞浆菌病的76%的患者中可见,而H条带仅为20%。但H条带常提示严重的急性肺部感染,播散性感染和空洞型疾病。[22]Wheat LJ. Improvements in diagnosis of histoplasmosis. Expert Opin Biol Ther. 2006;6:1207-1221.http://www.ncbi.nlm.nih.gov/pubmed/17049017?tool=bestpractice.com
在艾滋病患者中,血清学检测敏感性降至70%。[2]Wheat LJ, Connolly-Stringfield PA, Baker RL, et al. Disseminated histoplasmosis in the acquired immune deficiency syndrome: clinical findings, diagnosis and treatment, and review of the literature. Medicine (Baltimore). 1990;69:361-374.http://www.ncbi.nlm.nih.gov/pubmed/2233233?tool=bestpractice.com
血清学(抗体检测):补体结合试验
这项检测比免疫扩散试验的敏感性更高(95% vs. 90%),并且速度更快。 然而,该检测的特异性由于其它真菌感染(球孢子菌,芽生菌)的交叉反应而有所降低。[29]Wheat J, French ML, Kohler RB, et al. The diagnostic laboratory tests for histoplasmosis: analysis of experience in a large urban outbreak. Ann Intern Med. 1982;97:680-685.http://www.ncbi.nlm.nih.gov/pubmed/6814316?tool=bestpractice.com
它使用荚膜组织胞浆菌酵母型和菌丝型抗原。
全血细胞计数
肝功能检查
活检
当患者被评估为真菌感染可能高,而血清学检测阴性或可疑阳性时,组织活检发现组织病理学的证据可以协助诊断。 [Figure caption and citation for the preceding image starts]: 六胺银染色显示荚膜组织胞浆菌肺组织中的真菌Edwin P. Ewing, Jr 医生,美国疾病预防控制中心公共健康图片库 [Citation ends].
[Figure caption and citation for the preceding image starts]: 六胺银染色显示荚膜组织胞浆菌肺组织中的真菌Edwin P. Ewing, Jr 医生,美国疾病预防控制中心公共健康图片库 [Citation ends]. [Figure caption and citation for the preceding image starts]: 肺组织胞浆菌的组织病理学改变。Martin Hicklin 医生,美国疾病预防控制中心公共健康图片库 [Citation ends].
[Figure caption and citation for the preceding image starts]: 肺组织胞浆菌的组织病理学改变。Martin Hicklin 医生,美国疾病预防控制中心公共健康图片库 [Citation ends].
典型试验室表现
急性肺组织胞浆菌病(症状<4周)
急性肺组织胞浆菌病(症状>4周 )
慢性肺组织胞浆菌病
播散性感染
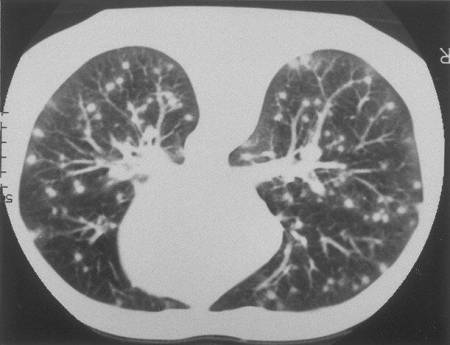 [Figure caption and citation for the preceding image starts]: 肺部CT示典型的急性组织胞浆菌感染的“暴风雪样”改变。美国疾病预防控制中心公共健康图片库 [Citation ends].
[Figure caption and citation for the preceding image starts]: 肺部CT示典型的急性组织胞浆菌感染的“暴风雪样”改变。美国疾病预防控制中心公共健康图片库 [Citation ends].