治疗方案分为微生物职业暴露的治疗、初级预防、活动性疾病治疗和二级预防。大多数感染此病的健康人群症状较轻且有自限性,并不需要治疗(除眼病患者外)。
职业暴露
为一群通过接触被感染的血液或细胞培养物而暴露于刚地弓形虫的人群。
其患病风险应根据暴露类型(深度针刺与针刺)、微生物负荷量(高浓度和体液低负荷)和基因型(毒性 I 型菌株与其他菌株)来进行分层。
应对此类患者立即行弓形虫 IgG 抗体检查以确定其是否有急性感染风险。
所有血清学阴性或未知的疾病暴露患者都应接受治疗。大多数专家会对所有有明确暴露的人群进行治疗。
对于那些检测不到抗体的人群,其治疗应持续 4 周且应对其再次行血清检测。如果患者出现血清转换,则应进行临床随访。对于初始治疗时血清反应阳性的患者,或在疾病暴露前已知其血清为阳性的患者,可能已有部分保护。大多数专家将对高度暴露于毒性 I 型菌株的患者进行2 周的治疗。(I 型菌株 [RH, GT-1] 为实验室常用菌株,其对老鼠有高度致命性。在免疫功能正常的个体,这些基因型曾引起过视网膜炎和其他严重的症状性感染的暴发。)
治疗的益处包括预防急性感染。风险包括药物的副作用。
对于在使用弓形虫的机构工作的女性,应对其基线时的血清学进行检查。如果结果为阴性,在妊娠或打算受孕期间应避免暴露。
值得注意的是:目前尚无已发布的关于职业暴露相关治疗的指南或试验。
HIV 患者的预防
对于免疫力低下患者,应对其进行预防治疗以防止潜伏性感染的再次激活。[41]Siberry GK, Abzug MJ, Nachman S, et al. Guidelines for the prevention and treatment of opportunistic infections in HIV-exposed and HIV-infected children: recommendations from the National Institutes of Health, Centers for Disease Control and Prevention, the HIV Medicine Association of the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the American Academy of Pediatrics. Pediatr Infect Dis J. 2013;32 (Suppl 2):i-KK4.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4169043/http://www.ncbi.nlm.nih.gov/pubmed/24569199?tool=bestpractice.com
所有 HIV 感染且 CD4+ T 淋巴细胞计数<100 个/μL的成人和大于 6 岁的儿童,以及所有 CD4%<15% 的 HIV 感染的 6 岁以下儿童,如果检测出弓形虫 IgG 抗体,均应接受初级预防,同时那些未检测出 IgG 抗体的患者,应接受关于避免将来感染(避免食用未煮熟的肉或接触猫的粪便)的指导。[22]Department of Health and Human Services Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. 2016. http://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf (last accessed 1 July 2016)https://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf[41]Siberry GK, Abzug MJ, Nachman S, et al. Guidelines for the prevention and treatment of opportunistic infections in HIV-exposed and HIV-infected children: recommendations from the National Institutes of Health, Centers for Disease Control and Prevention, the HIV Medicine Association of the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the American Academy of Pediatrics. Pediatr Infect Dis J. 2013;32 (Suppl 2):i-KK4.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4169043/http://www.ncbi.nlm.nih.gov/pubmed/24569199?tool=bestpractice.com
一线预防药物为甲氧苄啶/磺胺甲噁唑,每日服用 1 片(双倍加强片剂)。这也是耶氏肺孢子虫(卡氏肺囊虫)肺炎的预防药物。此方案不能用于治疗活动性疾病,因其有较高的治疗失败的风险。药物副作用包括皮疹、发热、白细胞减少、血小板减少症和肝毒性。
如果患者对磺胺类药物过敏或出现相关毒性症状(有高达 20% 的 HIV 阳性患者可出现磺胺类药剂相关的皮疹症状),则可选择的替代性预防药物包括:每日服用氨苯砜加每周一次服用乙胺嘧啶和亚叶酸钙;或每周一次氨苯砜、乙胺嘧啶和亚叶酸钙;或每日一次阿托伐醌加或不加乙胺嘧啶和亚叶酸钙。[22]Department of Health and Human Services Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. 2016. http://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf (last accessed 1 July 2016)https://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf
如果患者正接受抗逆转录病毒治疗 (ART) 且其 CD4+ T 淋巴细胞计数维持在 200 个细胞/μL 以上持续 3 个月或更长时间,则可停止初级预防治疗。[22]Department of Health and Human Services Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. 2016. http://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf (last accessed 1 July 2016)https://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf目前HIV感染儿童停止初级预防的安全性尚无研究。
移植受者的预防
在实体器官移植中,当血清学反应阴性的受者接受血清学反应阳性捐赠者的心脏移植时,应予以预防治疗。建议在移植后的前 3 个月使用乙胺嘧啶加磺胺嘧啶加亚叶酸钙,随后终身使用乙胺嘧啶和甲氧苄啶/磺胺甲噁唑。替代疗法可包括氨苯砜加乙胺嘧啶或阿托伐醌加或不加乙胺嘧啶,其可被用作初级治疗方案。有些中心对使用磺胺类药物过敏的患者采用单独乙胺嘧啶进行治疗。如果使用乙胺嘧啶来预防骨髓抑制,则应始终对患者加服亚叶酸钙进行治疗。[25]Parasitic infections. Am J Transplant. 2004;4(suppl 10):142-155.http://onlinelibrary.wiley.com/doi/10.1111/j.1600-6135.2004.00677.x/fullhttp://www.ncbi.nlm.nih.gov/pubmed/15504227?tool=bestpractice.com
在造血干细胞移植 (HSCT) 受者,应对有活动性移植物抗宿主病的血清学反应阳性的异基因 HSCT 受者,或有弓形体性脉络膜视网膜炎病史的受者实施预防治疗。[26]Tomblyn M, Chiller T, Einsele H, et al. Guidelines for preventing infectious complications among hematopoietic cell transplantation recipients: a global perspective. Biol Blood Marrow Transplant. 2009;15:1143-1238.http://www.bbmt.org/article/S1083-8791(09)00300-0/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/19747629?tool=bestpractice.com移植后应立即开始预防治疗,且只要患者在接受免疫抑制治疗,此预防治疗应一直持续。与每日服用甲氧苄啶/磺胺甲噁唑相比,非每日服用甲氧苄啶/磺胺甲噁唑患者出现突破疾病的更多。对于不能耐受甲氧苄啶/磺胺甲噁唑的患者,可对其使用克林霉素加乙胺嘧啶加亚叶酸钙。[26]Tomblyn M, Chiller T, Einsele H, et al. Guidelines for preventing infectious complications among hematopoietic cell transplantation recipients: a global perspective. Biol Blood Marrow Transplant. 2009;15:1143-1238.http://www.bbmt.org/article/S1083-8791(09)00300-0/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/19747629?tool=bestpractice.com
对有活动性感染的免疫功能低下患者的治疗
治疗目的是预防播散性疾病导致的死亡,以及防止/限制疾病对特异性器官的损害。[41]Siberry GK, Abzug MJ, Nachman S, et al. Guidelines for the prevention and treatment of opportunistic infections in HIV-exposed and HIV-infected children: recommendations from the National Institutes of Health, Centers for Disease Control and Prevention, the HIV Medicine Association of the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the American Academy of Pediatrics. Pediatr Infect Dis J. 2013;32 (Suppl 2):i-KK4.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4169043/http://www.ncbi.nlm.nih.gov/pubmed/24569199?tool=bestpractice.com应在乙胺嘧啶加磺胺嘧啶加亚叶酸钙治疗之前,给予一次负荷剂量的乙胺嘧啶。这些药物无静脉使用制剂。如果患者对磺胺嘧啶治疗的敏感性增加,则可给予患者克林霉素代替磺胺嘧啶进行治疗。其他治疗方案包括甲氧苄啶/磺胺甲噁唑、阿托伐醌加乙胺嘧啶加亚叶酸钙、阿托伐醌加磺胺嘧啶、阿托伐醌单独使用以及乙胺嘧啶加阿奇霉素加亚叶酸钙。[22]Department of Health and Human Services Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. 2016. http://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf (last accessed 1 July 2016)https://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf由于以上替代治疗方案还未进行过严格的研究,因此应在传染病专家的指导下使用。
所有免疫功能低下患者的初始治疗时间应持续 6 周,但如果在治疗期间中枢神经系统病变无明显改善,则其治疗时间应延长。[22]Department of Health and Human Services Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. 2016. http://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf (last accessed 1 July 2016)https://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf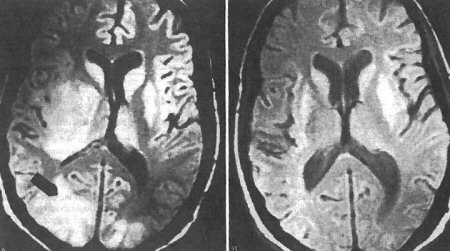 [Figure caption and citation for the preceding image starts]: 对于中枢神经系统弓形虫病治疗前后的脑部 MRI本文由 Rima L. McLeod 博士提供;经授权使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: 对于中枢神经系统弓形虫病治疗前后的脑部 MRI本文由 Rima L. McLeod 博士提供;经授权使用 [Citation ends].
对于移植受者,在允许的情况下,应尽量减少免疫抑制治疗。[25]Parasitic infections. Am J Transplant. 2004;4(suppl 10):142-155.http://onlinelibrary.wiley.com/doi/10.1111/j.1600-6135.2004.00677.x/fullhttp://www.ncbi.nlm.nih.gov/pubmed/15504227?tool=bestpractice.com如果在治疗 1 周后,临床或放射影像提示病情恶化(如脑炎患者脑部病变面积扩大),或在治疗 2 周后,临床或放射影像未提示有病情改善,则表明治疗失败。如发生此情况,应对患者进行脑活检。如随后的脑活检证实患者有弓形虫脑炎,应考虑将其治疗方法更换为替代治疗方案之一。[22]Department of Health and Human Services Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. 2016. http://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf (last accessed 1 July 2016)https://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf
在完成初始治疗后,只要患者免疫功能低下,则应继续接受二级预防治疗以防止感染再次激活。
疑似或被确诊有急性感染的妊娠患者
治疗目的是预防或限制未终止妊娠的胎儿感染的严重程度。尽管观察性队列研究显示治疗有益处,但没有相关的产前治疗的随机对照试验。[42]SYROCOT (Systematic Review on Congenital Toxoplasmosis) study group, Thiebaut R, Leproust S, et al. Effectiveness of prenatal treatment for congenital toxoplasmosis: a meta-analysis of individual patients' data. Lancet. 2007;369:115-122.http://www.ncbi.nlm.nih.gov/pubmed/17223474?tool=bestpractice.com
对于妊娠早期感染的女性,可采用螺旋霉素治疗以降低传播给胎儿的风险。[43]Daffos F, Forestier F, Capella-Pavlovsky M, et al. Prenatal management of 746 pregnancies at risk for congenital toxoplasmosis. N Engl J Med. 1988;318:271-275.http://www.ncbi.nlm.nih.gov/pubmed/3336419?tool=bestpractice.com应在第 10 周采集患者绒毛膜绒毛样本,或在第 15 周对患者进行羊膜穿刺术检查(直至结果出现之前应继续使用螺旋霉素)。在第 17 周应对胎儿采集血样检查。如果在早期妊娠后,未检测出胎儿有感染(羊水 PCR 阴性和/或胎儿血样 IgM 检测阴性),则可在出生前继续使用螺旋霉素。
估计螺旋霉素可减少 60% 的垂直感染发生率。[6]Montoya JG, Liesenfeld O. Toxoplasmosis. Lancet. 2004 Jun 12;363(9425):1965-76.http://www.ncbi.nlm.nih.gov/pubmed/15194258?tool=bestpractice.com值得注意的是,如果感染已经传染给胎儿,那么单独使用螺旋霉素无效。
如果已有宫内感染,则应开始进行治疗。乙胺嘧啶是一种有效的治疗方法,但由于其为叶酸拮抗物,且为潜在的致畸物,所以其只能被用于妊娠 21 周后的患者。如果妊娠 20 周之前胎儿感染,则应于 20 周前单独使用磺胺嘧啶治疗,然后加服乙胺嘧啶和亚叶酸钙。此项治疗方案可替代为螺旋霉素每月一次,以减少治疗对胎儿产生的毒性作用,或者直到胎儿出生前,对其一直使用螺旋霉素进行治疗。[29]Remington JS, McLeod R, Desmonts G. Toxoplasmosis. In: Infectious diseases of the fetus and newborn infant. JS Remington, JO Klein, eds. Philadelphia, PA: WB Saunders; 1995:chapter 5.在妊娠 21 周后,对患者的治疗应包括磺胺嘧啶/乙胺嘧啶,加亚叶酸钙和螺旋霉素交替使用,从而实现最小的毒性作用,达到最佳的治疗效果。[43]Daffos F, Forestier F, Capella-Pavlovsky M, et al. Prenatal management of 746 pregnancies at risk for congenital toxoplasmosis. N Engl J Med. 1988;318:271-275.http://www.ncbi.nlm.nih.gov/pubmed/3336419?tool=bestpractice.com
对于服用乙胺嘧啶的患者,应经常监测其血常规。如果出现巨幼红细胞性贫血、粒细胞减少症或血小板减少症,则应增加亚叶酸钙的使用量。[29]Remington JS, McLeod R, Desmonts G. Toxoplasmosis. In: Infectious diseases of the fetus and newborn infant. JS Remington, JO Klein, eds. Philadelphia, PA: WB Saunders; 1995:chapter 5.
先天性感染
治疗目标是预防或限制中枢神经系统和眼部的病理学改变。早期治疗(年龄小于 2.5 个月)且治疗持续 12 个月可产生较为可观的疗效,尤其可减少感音神经性听力受损的发生率。[29]Remington JS, McLeod R, Desmonts G. Toxoplasmosis. In: Infectious diseases of the fetus and newborn infant. JS Remington, JO Klein, eds. Philadelphia, PA: WB Saunders; 1995:chapter 5.[44]Brown ED, Chau JK, Atashband S, et al. A systematic review of neonatal toxoplasmosis exposure and sensorineural hearing loss. Int J Pediatr Otorhinolaryngol. 2009;73:707-711.http://www.ncbi.nlm.nih.gov/pubmed/19215990?tool=bestpractice.com
感染的新生儿应持续 1 年使用乙胺嘧啶加磺胺嘧啶加亚叶酸钙的治疗。[45]McLeod R, Boyer K, Karrison T, et al. Outcome of treatment for congenital toxoplasmosis, 1981-2004: the National Collaborative Chicago-Based, Congenital Toxoplasmosis Study. Clin Infect Dis. 2006;42:1383-1394.http://www.ncbi.nlm.nih.gov/pubmed/16619149?tool=bestpractice.com如果因胃肠道不良反应(恶心、呕吐)不能耐受口服药物或出现骨髓抑制,则可能需要减少乙胺嘧啶的剂量,并增加亚叶酸钙的剂量。
对磺胺类药物过敏的患者,替代性治疗方案包括乙胺嘧啶加亚叶酸钙,同时加服克林霉素、阿奇霉素或阿托伐醌(根据体重服用标准剂量。)[46]Roberts F, Kuo A, Jones L, et al. Ocular toxoplasmosis: clinical features, pathology, pathogenesis, animal models, and immune responses. In: Ajioka JW, Soldati D, eds. Toxoplasma molecular and cellular biology. Norfolk, UK: Horizon Bioscience; 2007:chapter 4.然而,临床数据非常有限,难以提供进一步建议。[29]Remington JS, McLeod R, Desmonts G. Toxoplasmosis. In: Infectious diseases of the fetus and newborn infant. JS Remington, JO Klein, eds. Philadelphia, PA: WB Saunders; 1995:chapter 5.此外,当患者脑脊液蛋白升高 (>10 g/L [1 g/dL]) 或出现影响视力的活动性脉络膜视网膜炎时,可同时给予其泼尼松龙和乙胺嘧啶磺胺嘧啶进行治疗。皮质类固醇应一直使用到脑脊液蛋白或活动性脉络膜视网膜炎恢复,随后应迅速逐渐减量。皮质类固醇仅可与乙胺嘧啶、磺胺嘧啶和亚叶酸钙共同使用。[29]Remington JS, McLeod R, Desmonts G. Toxoplasmosis. In: Infectious diseases of the fetus and newborn infant. JS Remington, JO Klein, eds. Philadelphia, PA: WB Saunders; 1995:chapter 5.
眼科疾病
治疗的目的是限制对眼部病变部位的损伤,同时缩短症状持续时间。 [Figure caption and citation for the preceding image starts]: 治疗视网膜脉络膜炎本文由 Rima L. McLeod 博士提供,并发表于:Roberts F、McLeod R. 的《视网膜脉络膜炎的发病学》。当代寄生虫学。1999;15:51-57;授权使用 [Citation ends].然而当前治疗弓形体性脉络膜视网膜炎的临床随机试验较少,且根据系统性综述,目前尚无证据支持常规抗生素治疗,免疫功能低下患者的任何病变、重度或持续性黄斑或视神经损伤、伴有重度炎症的大面积视网膜损伤和均需要治疗。[47]Gilbert RE, See SE, Jones LV, et al. Antibiotics versus control for toxoplasma retinochoroiditis. Cochrane Database Syst Rev. 2002;(1):CD002218.http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD002218/fullhttp://www.ncbi.nlm.nih.gov/pubmed/11869630?tool=bestpractice.com[48]Stanford MR, See SE, Jones LV, et al. Antibiotics for toxoplasmic retinochoroiditis: an evidence-based systematic review. Ophthalmology. 2003;110:926-932.http://www.ncbi.nlm.nih.gov/pubmed/12750091?tool=bestpractice.com[49]Jasper S, Vedula SS, John SS, et al. Corticosteroids as adjuvant therapy for ocular toxoplasmosis. Cochrane database Syst Rev. 2013;(4):CD007417.http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007417.pub2/fullhttp://www.ncbi.nlm.nih.gov/pubmed/23633342?tool=bestpractice.com对于免疫功能正常患者的小的、周边的眼底病变是否治疗,目前也存在争议。[46]Roberts F, Kuo A, Jones L, et al. Ocular toxoplasmosis: clinical features, pathology, pathogenesis, animal models, and immune responses. In: Ajioka JW, Soldati D, eds. Toxoplasma molecular and cellular biology. Norfolk, UK: Horizon Bioscience; 2007:chapter 4.
[Figure caption and citation for the preceding image starts]: 治疗视网膜脉络膜炎本文由 Rima L. McLeod 博士提供,并发表于:Roberts F、McLeod R. 的《视网膜脉络膜炎的发病学》。当代寄生虫学。1999;15:51-57;授权使用 [Citation ends].然而当前治疗弓形体性脉络膜视网膜炎的临床随机试验较少,且根据系统性综述,目前尚无证据支持常规抗生素治疗,免疫功能低下患者的任何病变、重度或持续性黄斑或视神经损伤、伴有重度炎症的大面积视网膜损伤和均需要治疗。[47]Gilbert RE, See SE, Jones LV, et al. Antibiotics versus control for toxoplasma retinochoroiditis. Cochrane Database Syst Rev. 2002;(1):CD002218.http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD002218/fullhttp://www.ncbi.nlm.nih.gov/pubmed/11869630?tool=bestpractice.com[48]Stanford MR, See SE, Jones LV, et al. Antibiotics for toxoplasmic retinochoroiditis: an evidence-based systematic review. Ophthalmology. 2003;110:926-932.http://www.ncbi.nlm.nih.gov/pubmed/12750091?tool=bestpractice.com[49]Jasper S, Vedula SS, John SS, et al. Corticosteroids as adjuvant therapy for ocular toxoplasmosis. Cochrane database Syst Rev. 2013;(4):CD007417.http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007417.pub2/fullhttp://www.ncbi.nlm.nih.gov/pubmed/23633342?tool=bestpractice.com对于免疫功能正常患者的小的、周边的眼底病变是否治疗,目前也存在争议。[46]Roberts F, Kuo A, Jones L, et al. Ocular toxoplasmosis: clinical features, pathology, pathogenesis, animal models, and immune responses. In: Ajioka JW, Soldati D, eds. Toxoplasma molecular and cellular biology. Norfolk, UK: Horizon Bioscience; 2007:chapter 4.
在免疫功能正常患者中,无论是先天还是获得性眼科疾病都应接受乙胺嘧啶、磺胺嘧啶、亚叶酸钙和泼尼松龙治疗。
皮质类固醇应用至炎症消退(通常为 1 到 2 周),随后迅速减量。在免疫功能正常患者的活动性感染的体征和症状消退后,继续使用乙胺嘧啶和磺胺嘧啶 1 到 2 周。在停止使用乙胺嘧啶后,应继续使用亚叶酸钙 1 周。尽管甲氧苄啶/磺胺甲噁唑对于疾病的慢性抑制有一定的效果,但疾病的复发率仍高达 10%,且目前尚无确认的预防复发的治疗方案。[46]Roberts F, Kuo A, Jones L, et al. Ocular toxoplasmosis: clinical features, pathology, pathogenesis, animal models, and immune responses. In: Ajioka JW, Soldati D, eds. Toxoplasma molecular and cellular biology. Norfolk, UK: Horizon Bioscience; 2007:chapter 4.[50]Silveira C, Belfort R, Muccioli C, et al. The effect of long-term intermittent trimethoprim/sulfamethoxazole treatment on recurrences of toxoplasmic retinochoroiditis. Am J Ophthalmol. 2002;134:41-46.http://www.ncbi.nlm.nih.gov/pubmed/12095806?tool=bestpractice.com[51]Kim SJ, Scott IU, Brown GC, et al. Interventions for toxoplasma retinochoroiditis: a report by the American Academy of Ophthalmology. Ophthalmology. 2013;120:371-378.http://www.ncbi.nlm.nih.gov/pubmed/23062648?tool=bestpractice.com
对于仅有眼科疾病的免疫功能低下患者,应接受上述治疗方案,并在他们随后的免疫受抑制期间,予以长期抑制方案。
预防复发
对于已完成弓形虫病初始治疗的免疫抑制患者,除非 HIV 感染患者经 ART 治疗后出现免疫重建或停用免疫抑制药物,否则其应继续接受终身二级预防治疗。由于长期维持治疗需要予以多种不同剂量方案的药物,因此对于患者来说,遵守长期治疗方案较为困难。
推荐的二级预防治疗方案为乙胺嘧啶加磺胺嘧啶加亚叶酸钙。替代性二级预防的治疗方案(对磺胺类药物过敏的患者)包括克林霉素加乙胺嘧啶加亚叶酸钙,或阿托伐醌加或不加乙胺嘧啶和亚叶酸钙。[22]Department of Health and Human Services Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. 2016. http://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf (last accessed 1 July 2016)https://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf
如果在开始 ART 后,出现免疫重建,且伴有持续 6 个月或更长时间的 CD4+ T 淋巴细胞计数>200 个细胞/μL,则应考虑停止长期维持治疗。目前停止儿童维持治疗的安全性尚无研究。
