怀疑急性冠状动脉综合征的患者需要紧急评估。关键是鉴别症状是否为急性冠状动脉综合征的表现,如果是,发生临床不良事件的风险有多高。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com医生首先需要确定患者的风险,并依据现行指南的初始风险评估,选择合适的管理策略。初始风险评估包括病史、查体、心电图和心脏生物标志物。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com[35]National Institute for Health and Care Excellence. Chest pain of recent onset: assessment and diagnosis. November 2016. http://www.nice.org.uk/guidance/CG95 (last accessed 28 July 2017).http://www.nice.org.uk/guidance/CG95http://www.ncbi.nlm.nih.gov/pubmed/20538674?tool=bestpractice.com
心电图(ECG)
心电图应当作为所有患者的一线检查,不能因为询问病史、体检或进行其他诊断性检查而延迟。应在患者到达急诊机构 10 分钟内进行 12 导联心电图检查并做出解释。排除ST段抬高型心肌梗死对于即刻实施治疗至关重要。非ST段抬高型心肌梗死与急性冠状动脉综合征其他类型(ST段抬高型心肌梗死或不稳定型心绞痛)很难鉴别,因为其病理生理和表现相似,只有心电图和生物标志物可以帮助鉴别。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com可能有典型心电图表现,但是许多患者就诊时心电图正常,因此初期需以 15-30 分钟间隔进行连续心电图检查,以观察发生 ST 段抬高或压低的可能性。非 ST 段抬高型心肌梗死的典型心电图缺血表现包括 ST 段水平或下斜型压低>0.5 mm 和/或对称性的 T 波倒置>2.0 mm。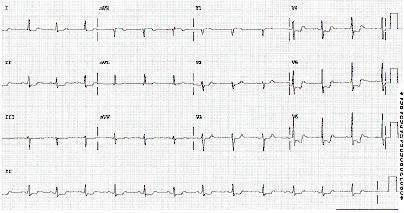 [Figure caption and citation for the preceding image starts]: 心电图显示ST段压低来源:休斯顿德克萨斯大学心内科医生 Syed W. Yusuf 博士和 Iyad N. Daher 博士;经允许后使用。 [Citation ends].
[Figure caption and citation for the preceding image starts]: 心电图显示ST段压低来源:休斯顿德克萨斯大学心内科医生 Syed W. Yusuf 博士和 Iyad N. Daher 博士;经允许后使用。 [Citation ends].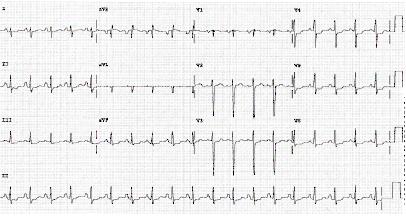 [Figure caption and citation for the preceding image starts]: 心电图显示ST段压低来源:休斯顿德克萨斯大学心内科医生 Syed W. Yusuf 博士和 Iyad N. Daher 博士;经允许后使用。 [Citation ends].
[Figure caption and citation for the preceding image starts]: 心电图显示ST段压低来源:休斯顿德克萨斯大学心内科医生 Syed W. Yusuf 博士和 Iyad N. Daher 博士;经允许后使用。 [Citation ends].
如果初始心电图不能诊断,持续12导联心电图监测可作为系列12导联心电图的合理替代检查。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com对于初始心电图不能诊断的患者,添加V7至V9导联有助于排除左回旋支闭塞导致的心肌梗死。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com少数情况下,心电图可以发现心肌梗死导致的心动过速或心动过缓。
病史和体格检查
对于因胸痛或不适前来就诊的患者,需要立即评估冠状动脉疾病 (CAD) 的现病史或既往史以及传统危险因素(例如年龄、性别、糖尿病、高血压 [HTN]、可卡因的使用),以区分需要优先治疗的患者。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com如果有胸痛史或左臂痛与既往记录的心绞痛相似并有冠状动脉疾病史(包括心肌梗死),则很可能是急性冠状动脉综合征。心绞痛典型表现为深层、难定位的胸痛或手臂痛,有紧缩感、沉重感、酸痛、烧灼痛、压迫感和压榨痛。疼痛最常位于胸骨后,常放射至左臂、也可能放射至下颌、颈部、双臂、后背以及上腹部,类似烧心症状。通常与劳累和情绪紧张相关(偶与暴露于寒冷环境相关),并且休息或舌下含服硝酸甘油可以缓解。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com
出汗是常见症状。呼吸急促也很常见,很可能是继发于心输出量降低。患者表达或表现焦虑。他们可能会描述有濒死感。典型情况下,上午 8 点钟左右是发作高峰期,原因可能是血清皮质醇、肾上腺激素、血小板聚集水平增高,引起血液动力学压力。
患者可能有各种不典型症状,其中任何一种都可能是唯一症状。这些症状包括乏力、恶心、呕吐、腹痛以及晕厥。这些在女性患者、老年人和糖尿病或慢性肾病患者中更常见。查体通常没有特异性发现,可能发现高血压或低血压,听诊可闻及第三、第四心音和第二心音反常分裂。可能观察到心力衰竭体征(颈静脉充盈,双肺听诊水泡爆裂音)或心源性休克表现,提示预后较差。
初始检查(非心电图)
除了心电图,所有患者均应当做以下检查。
舌下含服硝酸甘油尝试性治疗:患者进行性缺血不适应当接受试验性舌下含服硝酸甘油 (0.4 mg) 治疗,每 5 分钟一次,共给药 3 次,如无禁忌证,该治疗后应评估静脉使用硝酸甘油的需求。
心脏肌钙蛋白或其他心脏标志物:心脏肌钙蛋白水平升高(>正常值的第99百分位数)符合诊断条件。心脏肌钙蛋白水平在初始检测时是正常的,应当在6~8 h后重复检测。绝大多数医院都可以进行该项检查。如果不能,其他心脏标志物[CK,CK-MB 和(或)肌红蛋白]的典型升高和降低也可用于诊断。如果对患者的怀疑指数很高,但是系列心电图和心肌酶结果均为阴性,应当通过遥测设备或在胸痛病房接受密切监测,因为心脏标志物水平升高需要时间。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com
如果患者最近接受了经皮冠状动脉介入治疗,介入治疗后最初 48 小时内肌钙蛋白升高 5 倍以上,且具备以下任一项,则认为是 NSTEMI:[3]Thygesen K, Alpert JS, Jaffe AS, et al; the Writing Group on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Third universal definition of myocardial infarction. Circulation. 2012;126:2020-2035.http://circ.ahajournals.org/content/126/16/2020.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/22923432?tool=bestpractice.com
如果患者已行冠状动脉旁路移植术 (CABG),介入治疗后最初 48 小时内肌钙蛋白比正常基线水平升高超过 10 倍,且具备以下任一项,则考虑 NSTEMI:[3]Thygesen K, Alpert JS, Jaffe AS, et al; the Writing Group on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Third universal definition of myocardial infarction. Circulation. 2012;126:2020-2035.http://circ.ahajournals.org/content/126/16/2020.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/22923432?tool=bestpractice.com
胸部 X 线检查:适用于判定是否有充血性心力衰竭 (CHF),以及排除胸痛的非心源性病因。
全血细胞计数:血红蛋白和红细胞压积检查有助于评价非ST段抬高型心肌梗死的次要原因(如急性失血,贫血),并检查有无血小板减少症,评价出血风险。
尿素和血清肌酐:非ST段抬高型心肌梗死患者应当评估肌酐清除率,并且应适当调整经肾清除药物的剂量。对于慢性肾病患者,血管造影时首选等渗造影剂。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com[36]Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to update the 2001 guidelines for percutaneous coronary intervention). Circulation. 2006;113:e166-e286.http://circ.ahajournals.org/cgi/reprint/113/7/e166http://www.ncbi.nlm.nih.gov/pubmed/16490830?tool=bestpractice.com[4]Roffi M, Patrono C, Collet JP, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016;37:267-315.http://eurheartj.oxfordjournals.org/content/37/3/267.longhttp://www.ncbi.nlm.nih.gov/pubmed/26320110?tool=bestpractice.com
血清电解质:电解质紊乱可以导致心律失常。
肝功能检查:如果考虑使用经肝脏代谢的药物,则需要检查肝功能。
风险分层
管理急性冠状动脉综合征需要对死亡或复发性心肌梗死进行持续的风险分层。美国心脏病学会/美国心脏协会建议,疑似急性冠状动脉综合征患者依据急性冠状动脉综合征和不良结局发生的可能性进行风险分层,以进一步分类并协助选择治疗方案。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com当前已有许多风险评分,这些评分纳入了包括临床病史、心绞痛症状和同等症状、体格检查、心电图、肾功能和肌钙蛋白水平等在内的一些指标。可根据这些指标来估计死亡和非致死性心脏缺血性事件的风险,例如使用 TIMI 风险评分TIMI Risk Score calculator或 GRACE 风险模型。GRACE risk score calculator[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com[37]Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA. 2000;284:835-842.http://jama.jamanetwork.com/article.aspx?articleid=192996http://www.ncbi.nlm.nih.gov/pubmed/10938172?tool=bestpractice.com
TIMI 风险评分包括 7 个根据临床表现评定的风险指标。以下每1项表现记为1分:
年龄>65 岁
有≥3 个冠状动脉疾病危险因素
既往冠状动脉狭窄>50%
心电图ST段偏移
血清心脏生物标志物升高
在过去24 h,至少发作2次心绞痛
在过去7 d使用了阿司匹林。
患者TIMI评分0到2分为低危,3到4分为中危,5到7分为高危。14 天的全因死亡率、心肌梗死率和紧急血运重建率随 TIMI 评分中的危险因素数量增加而按比例增加。
GRACE 风险模型是一种基于网络的工具,可用于预测初次急性冠状动脉综合征后患者的住院和出院后死亡率或心肌梗死发生率。
Killip 分级是另一个用于风险分层的工具。该分级体系依据左心室衰竭的临床证据对急性心肌梗死患者进行风险分层:
Ⅰ级:没有慢性心力衰竭证据
Ⅱ级:出现第三心音奔马律、肺底啰音或颈静脉压升高
Ⅲ级:出现肺水肿
Ⅳ级:心源性休克。
HEART 评分纳入了患者病史、心电图、年龄、危险因素和肌钙蛋白等要素,用于急诊室环境中的患者,以评估急性心肌梗死、经皮冠状动脉介入治疗 (PCI)、CABG 和初次就诊后 6 周内死亡的风险。[38]Backus BE, Six AJ, Kelder JC, et al. A prospective validation of the HEART score for chest pain patients at the emergency department. Int J Cardiol. 2013;168:2153-2158.http://www.internationaljournalofcardiology.com/article/S0167-5273(13)00315-X/fulltexthttp://www.ncbi.nlm.nih.gov/pubmed/23465250?tool=bestpractice.com
后续检测
最初的病情检查及风险分层后,可考虑进行一些附加检查。
B型利钠肽(BNP)或N末端B型利钠肽原(NT-pro-BNP):BNP或NT-pro-BNP检测可以补充评价怀疑急性冠状动脉综合征患者的全心风险,特别是1型心肌梗死相关的心源性休克。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com
检测血脂:应当在入院最初的 24 小时内评估是否有脂质异常,以此决定是否需要降脂治疗。
血管造影:如果患者经强化药物治疗后仍不稳定,应当立即行紧急血管造影。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com适应证包括症状复发(难治性心绞痛),尽管予以充分药物治疗仍有缺血,高危(例如充血性心力衰竭、恶性室性心律失常),或无创检查的发现(显著左室功能不全、射血分数<0.35、大范围前壁或多处灌注缺损)。有严重过敏反应或造影剂过敏病史的患者必须在血管造影术前预先用药。 [Figure caption and citation for the preceding image starts]: 64层CT血管造影(A)和传统血管造影(B)显示右冠状动脉中段高度病变(箭头)。三角形指示的是可能被误认为病变的伪影。来源:Schussler JM and Grayburn PA. Heart, 2007;93:290-297 [Citation ends].
[Figure caption and citation for the preceding image starts]: 64层CT血管造影(A)和传统血管造影(B)显示右冠状动脉中段高度病变(箭头)。三角形指示的是可能被误认为病变的伪影。来源:Schussler JM and Grayburn PA. Heart, 2007;93:290-297 [Citation ends]. [Figure caption and citation for the preceding image starts]: 1例稳定型心绞痛患者的64层CT血管造影三维重构(A)、曲面重建图片(B)及传统造影证实的高度病变(C)。三角形指示部位为钙化斑块。Dx= 诊断来源:Schussler JM and Grayburn PA. Heart, 2007;93:290-297 [Citation ends].
[Figure caption and citation for the preceding image starts]: 1例稳定型心绞痛患者的64层CT血管造影三维重构(A)、曲面重建图片(B)及传统造影证实的高度病变(C)。三角形指示部位为钙化斑块。Dx= 诊断来源:Schussler JM and Grayburn PA. Heart, 2007;93:290-297 [Citation ends].
超声心动图:心脏超声对评价缺血并发症和其他原因的胸痛(如肺栓塞、积液、急性瓣膜病)都十分有用,初始评价后建议进行。心脏超声可以在心电图变化出现之前证明有缺血性改变。室壁节段运动异常以及左心室功能降低可以为急性冠状动脉综合征提供依据。同样重要的是,正常心脏功能和活力的阴性预测值很高,几乎可排除急性心肌梗死。因此,超声心动图有助于对怀疑心肌梗死的患者进行早期分类。[3]Thygesen K, Alpert JS, Jaffe AS, et al; the Writing Group on behalf of the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Third universal definition of myocardial infarction. Circulation. 2012;126:2020-2035.http://circ.ahajournals.org/content/126/16/2020.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/22923432?tool=bestpractice.com
负荷试验:包括平板运动试验在内的负荷试验可能有用,建议在(心电图正常且高敏感生物标志物正常的)验前概率为低度和中度的患者中进行,以帮助指导是否需要实施介入治疗。[1]Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139-e228.http://circ.ahajournals.org/content/130/25/e344.full.pdf+htmlhttp://www.ncbi.nlm.nih.gov/pubmed/25260718?tool=bestpractice.com[39]Lindahl B, Andren B, Ohlsson J, et al. Risk stratification in unstable coronary artery disease. Additive value of troponin T determinations and pre-discharge exercise tests. Eur Heart J. 1997;18:762-770.http://www.ncbi.nlm.nih.gov/pubmed/9152646?tool=bestpractice.com[40]Nyman I, Larsson H, Areskog M, et al. The predictive value of silent ischemia at an exercise test before discharge after an episode of unstable coronary artery disease. Am Heart J. 1992;123:324-331.http://www.ncbi.nlm.nih.gov/pubmed/1736566?tool=bestpractice.com 当与核成像结合观察心肌灌注有无缺损或与超声心动图结合评价室壁节段运动是否异常,负荷试验的敏感性和特异性提高。核成像负荷试验的关键性阳性发现是出现可逆缺损。这部分心肌区域在心肌需氧量增加时灌注明显减少,而在停止活动时出现再灌注。提示存在冠状动脉狭窄,可采用经皮冠状动脉介入治疗或冠状动脉旁路移植术治疗。于心肌梗死后 4-7 天进行亚极量运动试验,而症状限制性试验可于心肌梗死后 14-21 天进行,患者当时应无活动性缺血或心力衰竭症状。[41]Fletcher GF, Ades PA, Kligfield P, et al. Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation. 2013;128:873-934.http://circ.ahajournals.org/content/128/8/873.longhttp://www.ncbi.nlm.nih.gov/pubmed/23877260?tool=bestpractice.com
冠状动脉 CT 血管造影 (coronary CT angiography, CCTA):可以提供冠状动脉解剖结构和动脉粥样硬化的无创评估。肾功能衰竭是一个相对禁忌证。有造影剂过敏的患者可能需要在血管造影术前预先用药。[42]Raff GL, Gallagher MJ, O'Neill WW, et al. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography J Am Coll Cardiol. 2005;46:552-557.http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6T18-4GFV5KY-G&_user=10&_rdoc=1&_fmt=&_orig=search&_sort=d&view=c&_acct=C000050221&_version=1&_urlVersion=0&_userid=10&md5=905a4d1354efb369816f82eddeaf88b3http://www.ncbi.nlm.nih.gov/pubmed/16053973?tool=bestpractice.com由于冠状动脉CT血管造影的阴性预测值高,证据表明其对于低至中危的非ST段抬高型心肌梗死患者是有用的。与对低至中危患者的标准治疗(观察,系列酶学检查后行负荷试验)比较,冠状动脉CT血管造影缩短诊断时间,减少急诊科停留时间,并且安全性相似。[43]Hoffmann U, Truong QA, Schoenfeld DA, et al; ROMICAT-II Investigators. Coronary CT angiography versus standard evaluation in acute chest pain. N Engl J Med. 2012;367:299-308.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3662217/pdf/nihms405222.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/22830462?tool=bestpractice.com冠状动脉CT血管造影不应用于有高危特征的患者(即缺血性心电图改变,阳性心脏标志物)。[44]Hendel RC, Patel MR, Kramer CM, et al; American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group; American College of Radiology; Society of Cardiovascular Computed Tomography; Society for Cardiovascular Magnetic Resonance; American Society of Nuclear Cardiology; North American Society for Cardiac Imaging; Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology. ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol. 2006;48:1475-1497.http://ac.els-cdn.com/S0735109706017955/1-s2.0-S0735109706017955-main.pdf?_tid=4203aaa4-d077-11e5-b8a3-00000aacb361&acdnat=1455164813_0b21cb4b70845a55177b0c1e31df2e79http://www.ncbi.nlm.nih.gov/pubmed/17010819?tool=bestpractice.com[Figure caption and citation for the preceding image starts]: 1例稳定型心绞痛患者的64层CT血管造影三维重构(A)、曲面重建图片(B)及传统造影证实的高度病变(C)。三角形指示部位为钙化斑块。Dx= 诊断来源:Schussler JM and Grayburn PA. Heart, 2007;93:290-297 [Citation ends].[Figure caption and citation for the preceding image starts]: 64层CT血管造影(A)和传统血管造影(B)显示右冠状动脉中段高度病变(箭头)。三角形指示的是可能被误认为病变的伪影。来源:Schussler JM and Grayburn PA. Heart, 2007;93:290-297 [Citation ends].
