克罗恩病的临床表现和检查顺序视所累及的胃肠道部分、炎症的严重程度和存在的并发症而定。克罗恩病可能会累及从口腔到肛周部位的整个消化道的任何部分。通过典型的病史和查体发现可诊断克罗恩病,发现肛周受累则更有说服力。
病史
炎症性肠病的家族史会增加克罗恩病的患病可能性。白种人的患病率高于黑种人或亚洲人。德系犹太人患克罗恩病的风险高 2-4 倍。[1]Podolsky DK. Inflammatory bowel disease. N Engl J Med. 2002 Aug 8;347(6):417-29.http://www.ncbi.nlm.nih.gov/pubmed/12167685?tool=bestpractice.com[2]Ekbom A, Helmick C, Zack M, et al. The epidemiology of inflammatory bowel disease: a large, population-based study in Sweden. Gastroenterology. 1991 Feb;100(2):350-8.http://www.ncbi.nlm.nih.gov/pubmed/1985033?tool=bestpractice.com 发病高峰年龄为 15-40 岁,此外还有另一个较小的发病高峰为 60~80 岁。[2]Ekbom A, Helmick C, Zack M, et al. The epidemiology of inflammatory bowel disease: a large, population-based study in Sweden. Gastroenterology. 1991 Feb;100(2):350-8.http://www.ncbi.nlm.nih.gov/pubmed/1985033?tool=bestpractice.com 克罗恩病的临床表现包括各种症状组合,其中包括疲乏、腹泻、腹痛、体重下降、发热和胃肠道出血。许多患者会出现非特异性症状,并且许多年未得到确诊。
病史还应用来排除引起症状的其他病因。近期旅游、近期使用抗生素或患者接触提示为感染性腹泻的病因。肠结核 (Intestinal tuberculosis, TB) 是不应遗漏的重要诊断,因为将其误当成克罗恩病而采用免疫抑制治疗可危及患者生命。在高度疑似病例中,患者可能需要在专科医师指导下进行结核病经验性治疗。[33]Ooi CJ, Makharia GK, Hilmi I, et al. Asia Pacific consensus statements on Crohn's disease. Part 1: Definition, diagnosis, and epidemiology: (Asia Pacific Crohn's Disease Consensus - Part 1). J Gastroenterol Hepatol. 2016 Jan;31(1):45-55.http://onlinelibrary.wiley.com/doi/10.1111/jgh.12956/fullhttp://www.ncbi.nlm.nih.gov/pubmed/25819140?tool=bestpractice.com
体格检查
患者出现许多腹部体征,包括右下腹压痛和可触及的腹部肿块。此外,还应进行口腔溃疡检查、肛周皮赘的会阴检查、瘘管、脓肿和窦道检查以及潜血和肿块排除的直肠指检。应检查皮肤,以查找克罗恩病的肠外皮肤表现的体征,例如结节性红斑和坏疽性脓皮病。应计算体质指数 (BMI) 以作为未来体重变化的基线。 [Figure caption and citation for the preceding image starts]: 患者的手臂和手部出现结节性红斑CDC/ Margaret Renz [Citation ends].
[Figure caption and citation for the preceding image starts]: 患者的手臂和手部出现结节性红斑CDC/ Margaret Renz [Citation ends].
初始实验室检查
所有患者在初次就诊时都应进行全血细胞计数 (FBC)、综合代谢检查 (CMP)、C 反应蛋白 (CRP) 和红细胞沉降率 (ESR) 检查。他们还应进行血清铁检测以及维生素 B12 和叶酸水平检查。
应送交粪便进行显微镜检查(包括寄生虫卵、包囊和寄生虫成虫)和细菌培养。如果有近期抗生素使用史,表明须进行艰难梭菌毒素检查。临床疑似患有回肠炎的患者应进行回结肠耶尔森菌血清学检查。
影像学检查
初始检查应包括腹部 X 线平片。它们并不足以确诊克罗恩病,但可能具有提示作用,并有助于评估严重程度。或许可见肠袢扩张和气腹。
造影剂影像学检查(口服造影剂上消化道和小肠系列检查)往往被用于检查小肠克罗恩病。提示患有克罗恩病的检查结果包括黏膜下层水肿、僵硬、假憩室或瘘管。深层溃疡会导致肛周鹅卵石样表现。回肠炎可以表现为钡剂造影检查所示的线状病征,这种线状病征在痉挛或纤维化变窄之后继发。[4]Baumgart DC, Sandborn WJ. Inflammatory bowel disease: clinical aspects and established and evolving therapies. Lancet. 2007 May 12;369(9573):1641-57.http://www.ncbi.nlm.nih.gov/pubmed/17499606?tool=bestpractice.com[34]Rispo A, Imbriaco M, Celentano L, et al. Small bowel Crohn's disease: comparison of enteroclysis, bowel sonography and Tc-99m-HMPAO leukocyte scintigraphy. Eur Rev Med Pharmacol Sci. 2004 Sep-Oct;8(5):219-24.http://www.ncbi.nlm.nih.gov/pubmed/15638234?tool=bestpractice.com[35]Rubesin SE, Scotiniotis I, Birnbaum BA, et al. Radiologic and endoscopic diagnosis of Crohn's disease. Surg Clin North Am. 2001 Feb;81(1):39-70, viii.http://www.ncbi.nlm.nih.gov/pubmed/11218169?tool=bestpractice.com 尽管使用广泛,但是造影影像学检查已在很大程度上被 CT 和 MRI 取代作为首选的显像模式,后两者可以提供腹部器官和结构的更高分辨率成像和更多信息(例如淋巴结病和恶性肿瘤),以帮助医生进行诊断。
如果 CT 扫描尚未执行,且小肠 X 线检查不足以进行诊断,则表明须进行小肠 CT 扫描(静脉注射和口服造影剂)。禁忌使用造影剂时,可以采用 MRI。 [Figure caption and citation for the preceding image starts]: CT 扫描证实克罗恩病病情加重的患者的末端回肠增厚由 Wissam Bleibel、Bishal Mainali、Chandrashekhar Thukral 和 Mark A. Peppercorn 博士(本专题著作的前作者)合著 [Citation ends].
[Figure caption and citation for the preceding image starts]: CT 扫描证实克罗恩病病情加重的患者的末端回肠增厚由 Wissam Bleibel、Bishal Mainali、Chandrashekhar Thukral 和 Mark A. Peppercorn 博士(本专题著作的前作者)合著 [Citation ends].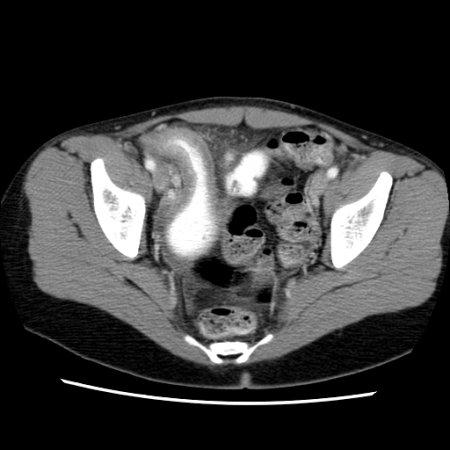 [Figure caption and citation for the preceding image starts]: CT 扫描证实克罗恩病病情加重的患者的末端回肠增厚由 Wissam Bleibel、Bishal Mainali、Chandrashekhar Thukral 和 Mark A. Peppercorn 博士(本专题著作的前作者)合著 [Citation ends].
[Figure caption and citation for the preceding image starts]: CT 扫描证实克罗恩病病情加重的患者的末端回肠增厚由 Wissam Bleibel、Bishal Mainali、Chandrashekhar Thukral 和 Mark A. Peppercorn 博士(本专题著作的前作者)合著 [Citation ends].
小肠和盆腔超声检查是 CT 扫描的替代性方案,如果疑似出现盆腔病变(例如脓肿),超声检查尤其有效。
无法进行结肠镜检查的患者可以进行锝-99 标记白细胞扫描,以便协助诊断。此项扫描可以突出显示炎症部位。在克罗恩病患者中,可能会显示胃肠炎症和跳跃性病变。此外,还将会检测到肠外炎症。
正电子发射断层成像 (PET) 使用氟-2-脱氧-D-葡萄糖 (FDG) 来确定代谢异常的部位。有证据表明该方法可以有效诊断糖酵解速率高的疾病,包括恶性肿瘤、感染和活动性炎症。它还可用作非侵入性检查,以早期检测无法耐受内镜检查评估的患者(例如儿童)是否患有克罗恩病。有研究表明,该方法对于检测肠道炎症的灵敏度非常高,但是特异性较差。[36]Spier BJ, Perlman SB, Reichelderfer M. FDG-PET in inflammatory bowel disease. Q J Nucl Med Mol Imaging. 2009 Feb;53(1):64-71.http://www.minervamedica.it/en/journals/nuclear-med-molecular-imaging/article.php?cod=R39Y2009N01A0064http://www.ncbi.nlm.nih.gov/pubmed/19182729?tool=bestpractice.com
内镜检查
结肠镜检查和回肠插管是克罗恩病诊断的确定性检查。[33]Ooi CJ, Makharia GK, Hilmi I, et al. Asia Pacific consensus statements on Crohn's disease. Part 1: Definition, diagnosis, and epidemiology: (Asia Pacific Crohn's Disease Consensus - Part 1). J Gastroenterol Hepatol. 2016 Jan;31(1):45-55.http://onlinelibrary.wiley.com/doi/10.1111/jgh.12956/fullhttp://www.ncbi.nlm.nih.gov/pubmed/25819140?tool=bestpractice.com 早期病变可见的口疮样溃疡会逐渐进展为更深的溃疡,进而累及整个结肠壁。这些溃疡之间的正常和炎症部位会形成克罗恩病的典型鹅卵石样表现。克罗恩病会以间断性方式累及肠道,引起跳跃性病变。支持克罗恩病诊断的其他特征包括直肠正常(可排除溃疡性结肠炎 [UC],因为溃疡性结肠炎通常累及直肠)和回肠末端孤立性受累。结肠炎和回肠炎的内窥镜检查结果包括红斑、水肿、脆性黏膜和检测到的瘘道口。 [Figure caption and citation for the preceding image starts]: 克罗恩回肠炎的内窥镜检查视图由 Wissam Bleibel、Bishal Mainali、Chandrashekhar Thukral 和 Mark A. Peppercorn 博士(本专题著作的前作者)合著 [Citation ends].
[Figure caption and citation for the preceding image starts]: 克罗恩回肠炎的内窥镜检查视图由 Wissam Bleibel、Bishal Mainali、Chandrashekhar Thukral 和 Mark A. Peppercorn 博士(本专题著作的前作者)合著 [Citation ends].
应对末端回肠和每段结肠进行肠黏膜活检,以寻找克罗恩病的显微镜检查证据。30-50% 的克罗恩病病例中可见非干酪性肉芽肿的透壁受累。[24]Heresbach D, Alexandre JL, Branger B, et al. Frequency and significance of granulomas in a cohort of incident cases of Crohn's disease. Gut. 2005 Feb;54(2):215-22.http://gut.bmj.com/content/54/2/215.longhttp://www.ncbi.nlm.nih.gov/pubmed/15647184?tool=bestpractice.com[25]Pierik M, De Hertogh G, Vermeire S, et al. Epithelioid granulomas, pattern recognition receptors, and phenotypes of Crohn's disease. Gut. 2005 Feb;54(2):223-7.http://www.ncbi.nlm.nih.gov/pubmed/15647186?tool=bestpractice.com 有助于鉴别溃疡性结肠炎和克罗恩病的显微镜特征包括肉芽肿、结构改变和疾病分布。[37]Feakins RM; British Society of Gastroenterology. Inflammatory bowel disease biopsies: updated British Society of Gastroenterology reporting guidelines. J Clin Pathol. 2013 Dec;66(12):1005-26.http://jcp.bmj.com/content/66/12/1005.longhttp://www.ncbi.nlm.nih.gov/pubmed/23999270?tool=bestpractice.com 如果正在考虑结核病,可以进行回盲部组织活检,检查是否有结核分枝杆菌。[33]Ooi CJ, Makharia GK, Hilmi I, et al. Asia Pacific consensus statements on Crohn's disease. Part 1: Definition, diagnosis, and epidemiology: (Asia Pacific Crohn's Disease Consensus - Part 1). J Gastroenterol Hepatol. 2016 Jan;31(1):45-55.http://onlinelibrary.wiley.com/doi/10.1111/jgh.12956/fullhttp://www.ncbi.nlm.nih.gov/pubmed/25819140?tool=bestpractice.com
应进行食管胃十二指肠镜检查 (OGD),以评估主要表现出上消化道症状的患者的病情。
影像学检查、结肠镜检查和食管胃十二指肠镜检查无法确诊时,应当考虑进行胶囊内窥镜检查。[33]Ooi CJ, Makharia GK, Hilmi I, et al. Asia Pacific consensus statements on Crohn's disease. Part 1: Definition, diagnosis, and epidemiology: (Asia Pacific Crohn's Disease Consensus - Part 1). J Gastroenterol Hepatol. 2016 Jan;31(1):45-55.http://onlinelibrary.wiley.com/doi/10.1111/jgh.12956/fullhttp://www.ncbi.nlm.nih.gov/pubmed/25819140?tool=bestpractice.com
免疫检查
在组织学未确定的炎症性肠病患者中,自身免疫抗体、核周型抗中性粒细胞胞质抗体 (p-ANCA) 和抗酿酒酵母甘露聚糖抗体 (ASCA) 可能有助于区分克罗恩病和溃疡性结肠炎,ASCA 阳性和 p-ANCA 阴性提示患有克罗恩病,反之则表明患有溃疡性结肠炎。然而,这些检查在临床上的诊断作用有限,因为其敏感性和特异性较低。[33]Ooi CJ, Makharia GK, Hilmi I, et al. Asia Pacific consensus statements on Crohn's disease. Part 1: Definition, diagnosis, and epidemiology: (Asia Pacific Crohn's Disease Consensus - Part 1). J Gastroenterol Hepatol. 2016 Jan;31(1):45-55.http://onlinelibrary.wiley.com/doi/10.1111/jgh.12956/fullhttp://www.ncbi.nlm.nih.gov/pubmed/25819140?tool=bestpractice.com
粪便钙卫蛋白和粪便乳铁蛋白
粪便钙卫蛋白和粪便乳铁蛋白是稳定蛋白,当任何消化道炎症部位出现中性粒细胞聚集时会被排放到粪便中。已将这两种蛋白作为肠道炎症的非侵入式标记物进行了大量研究。[38]van Rheenen PF, Van de Vijver E, Fidler V. Faecal calprotectin for screening of patients with suspected inflammatory bowel disease: diagnostic meta-analysis. BMJ. 2010 Jul 15;341:c3369.http://www.bmj.com/content/341/bmj.c3369http://www.ncbi.nlm.nih.gov/pubmed/20634346?tool=bestpractice.com[39]Kane SV, Sandborn WJ, Rufo PA, et al. Fecal lactoferrin is a sensitive and specific marker in identifying intestinal inflammation. Am J Gastroenterol. 2003 Jun;98(6):1309-14.http://www.ncbi.nlm.nih.gov/pubmed/12818275?tool=bestpractice.com 它们可能有助于鉴别非炎症性肠病(例如肠易激综合征)和炎症性肠病(IBD,例如克罗恩病)。它们还有助于预测无活动性炎症性肠病患者的复发和检测有症状患者的疾病活动,从而有可能避免具有侵入性的、需要大量资源的内镜监测。[40]Mao R, Xiao YL, Gao x, et al. Fecal calprotectin in predicting relapse of inflammatory bowel diseases: a meta-analysis of prospective studies. Inflamm Bowel Dis. 2012 Oct;18(10):1894-9.http://www.ncbi.nlm.nih.gov/pubmed/22238138?tool=bestpractice.com[41]Mosli MH, Zou G, Garg SK, et al. C-reactive protein, fecal calprotectin, and stool lactoferrin for detection of endoscopic activity in symptomatic inflammatory bowel disease patients: a systematic review and meta-analysis. Am J Gastroenterol. 2015 Jun;110(6):802-19.http://www.ncbi.nlm.nih.gov/pubmed/25964225?tool=bestpractice.com 在某些消化道恶性肿瘤(例如结直肠癌)和消化道感染病例中,钙卫蛋白和乳铁蛋白水平也可能会升高。特异性的缺乏会限制它们的诊断作用,尽管它们已被建议用作初级医疗保健中的筛查方法,以帮助确定哪些患者需要进行内镜检查评估。[42]Gisbert JP, McNicholl AG. Questions and answers on the role of faecal calprotectin as a biological marker in inflammatory bowel disease. Dig Liver Dis. 2009 Jan;41(1):56-66.http://www.ncbi.nlm.nih.gov/pubmed/18602356?tool=bestpractice.com[43]National Institute for Health and Care Excellence. Faecal calprotectin diagnostic tests for inflammatory diseases of the bowel. Oct 2013 [internet publication].http://www.nice.org.uk/guidance/dg11
