PJS患者通常在10岁或20岁内因息肉相关的肠梗阻就诊, 部分患者是因为家族病史就诊,进行症状性评估。
病史和家族史
几乎一半的患者表现出小肠梗阻。[2]Utsunomiya J, Gocho H, Miyanaga T, et al. Peutz-Jeghers syndrome: its natural course and management. Johns Hopkins Med J. 1975;136:71-82.http://www.ncbi.nlm.nih.gov/pubmed/1117595?tool=bestpractice.com 大约88%的PJS患者会出现息肉。[10]Giardiello FM, Trimbath JD. Peutz-Jeghers syndrome and management recommendations. Clin Gastroenterol Hepatol. 2006 Apr;4(4):408-15.http://www.ncbi.nlm.nih.gov/pubmed/16616343?tool=bestpractice.com 腹部不适和腹胀是最常见的症状。1/3 的患者在10 岁前就出现症状,将近一半的患者在 20 岁前出现症状,并因肠梗阻而需要接受手术。[2]Utsunomiya J, Gocho H, Miyanaga T, et al. Peutz-Jeghers syndrome: its natural course and management. Johns Hopkins Med J. 1975;136:71-82.http://www.ncbi.nlm.nih.gov/pubmed/1117595?tool=bestpractice.com[11]Tovar JA, Eizaguirre I, Albert A, et al. Peutz-Jeghers syndrome in children: report of two cases and review of the literature. J Pediatr Surg. 1983 Feb;18(1):1-6.http://www.ncbi.nlm.nih.gov/pubmed/6834218?tool=bestpractice.com[12]Spigelman AD, Thomson JP, Phillips RK. Towards decreasing the relaparotomy rate in the Peutz-Jeghers syndrome: the role of peroperative small bowel endoscopy. Br J Surg. 1990 Mar;77(3):301-2.http://www.ncbi.nlm.nih.gov/pubmed/2322793?tool=bestpractice.com 息肉可能会引起隐性或显性失血或者缺铁性贫血,患者可能诉有乏力。患者经常在出生时就有色素沉着,但是会随着时间推移而逐渐变浅。应注意患者或者家族有无任何肠内息肉、肠外息肉、皮肤黏膜色素沉着或恶性肿瘤的病史。
体格检查
PJS可以在口腔黏膜、嘴唇、口周、指端或脚趾出现特征性的色素沉着斑。[10]Giardiello FM, Trimbath JD. Peutz-Jeghers syndrome and management recommendations. Clin Gastroenterol Hepatol. 2006 Apr;4(4):408-15.http://www.ncbi.nlm.nih.gov/pubmed/16616343?tool=bestpractice.com皮肤色素沉着斑从婴儿和幼儿时期开始出现程度加重,但是成年后往往逐渐变浅,部分病例可以完全消退。口腔损害通常持续存在。[13]McGarrity TJ, Kulin HE, Zaino RJ. Peutz-Jeghers syndrome. Am J Gastroenterol. 2000 Mar;95(3):596-604.http://www.ncbi.nlm.nih.gov/pubmed/10710046?tool=bestpractice.com
虽然不常见,但继发于息肉的消化道出血仍可能导致贫血;苍白、乏力和心脏表现(心动过速、心脏杂音或心脏扩大)均可能出现。
男性需要检查是否存在睾丸肿瘤的信号。 睾丸轻度增大(没有包块)或者出现女性化性早熟特点(例如,男性乳房发育)提示可能有潜在滋养细胞肿瘤。 睾丸癌的诊断年龄在3岁到20岁,平均年龄为9岁。[1]Giardiello FM, Bresinger JD, Tersmette AC, et al. Very high risk of cancer in familial Peutz-Jeghers syndrome. Gastroenterology. 2000 Dec;119(6):1447-53.http://www.ncbi.nlm.nih.gov/pubmed/11113065?tool=bestpractice.com 偶尔息肉会经肛门脱出,男性和女性均可出现。 [Figure caption and citation for the preceding image starts]: 嘴唇和口腔黏膜上的特征性色素沉着手稿来自Carol A.Burke医生,并经过了他的同意 [Citation ends].
[Figure caption and citation for the preceding image starts]: 嘴唇和口腔黏膜上的特征性色素沉着手稿来自Carol A.Burke医生,并经过了他的同意 [Citation ends].
世界卫生组织 (WHO) 诊断标准
诊断PJS需要符合下列任意一条:[14]Aaltonen LA, Jarvin H, Gruber SB, et al. Peutz-Jeghers syndrome. In: Hamilton SR, Aaltonen LA, eds. Tumors of the digestive system. Lyon, France: IACR; 2000:74-6.http://www.iarc.fr/en/publications/pdfs-online/pat-gen/bb2/bb2-chap4.pdf
内镜评估
内镜评估用于三种人群:
应在 8 岁时开始进行小肠视频胶囊内镜检查、食管胃十二指肠镜检查 (oesophagogastroduodenoscopy, OGD) 和结肠镜检查。[15]Syngal S, Brand RE, Church JM, et al; American College of Gastroenterology. ACG clinical guideline: genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol. 2015 Feb;110(2):223-62.http://gi.org/wp-content/uploads/2015/02/ACG_Guideline_Hereditary-Gastrointestinal-Cancer-Syndromes_February_2015.pdfhttp://www.ncbi.nlm.nih.gov/pubmed/25645574?tool=bestpractice.com[16]Beggs AD, Latchford AR, Vasen HF, et al. Peutz-Jeghers syndrome: a systematic review and recommendations for management. Gut. 2010 Jul;59(7):975-86.http://www.ncbi.nlm.nih.gov/pubmed/20581245?tool=bestpractice.com对于曾行肠切除术的患者以及因小肠息肉引起轻度症状的患者,使用胶囊内镜是安全的。最常见的内镜下发现是弥漫的错构瘤性息肉。约 88% 的 PJS 患者会出现息肉。[10]Giardiello FM, Trimbath JD. Peutz-Jeghers syndrome and management recommendations. Clin Gastroenterol Hepatol. 2006 Apr;4(4):408-15.http://www.ncbi.nlm.nih.gov/pubmed/16616343?tool=bestpractice.com 小肠息肉(尤其是空肠息肉)最为常见,见于 75% 以上的患者。息肉较少发生在结肠 (42%)、胃 (38%) 和直肠 (28%) 等部位。[17]Hemminki A. The molecular basis and clinical aspects of Peutz-Jeghers syndrome. Cell Mol Life Sci. 1999 May;55(5):735-50.http://www.ncbi.nlm.nih.gov/pubmed/10379360?tool=bestpractice.com 一些罕见的病例,息肉也可以出现在肾盂、膀胱、肺脏和鼻孔。
息肉可大可小,有蒂或者无蒂。由于息肉内存在呈树枝状分布的平滑肌,故外观经常呈特征性的脑回样。通常为多发性息肉;总数通常低于 20。单个息肉的大小可从数毫米到数厘米不等。病理上,息肉的性质是错构瘤;以平滑肌为核心,周围是黏膜固有层和成熟的腺上皮。 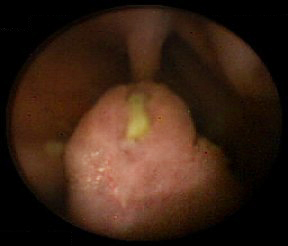 [Figure caption and citation for the preceding image starts]: 胶囊内镜可以发现小肠错构瘤息肉手稿来自Carol A.Burke医生,并经过了他的同意 [Citation ends].
[Figure caption and citation for the preceding image starts]: 胶囊内镜可以发现小肠错构瘤息肉手稿来自Carol A.Burke医生,并经过了他的同意 [Citation ends]. [Figure caption and citation for the preceding image starts]: 小肠内的息肉样包块手稿来自James Church医生,并经过了他的同意。 [Citation ends].[Figure caption and citation for the preceding image starts]: 胶囊内镜可以发现小肠错构瘤息肉手稿来自Carol A.Burke医生,并经过了他的同意 [Citation ends].
[Figure caption and citation for the preceding image starts]: 小肠内的息肉样包块手稿来自James Church医生,并经过了他的同意。 [Citation ends].[Figure caption and citation for the preceding image starts]: 胶囊内镜可以发现小肠错构瘤息肉手稿来自Carol A.Burke医生,并经过了他的同意 [Citation ends]. [Figure caption and citation for the preceding image starts]: PJS患者小肠有蒂错构瘤可见特征性的浆膜小凹。手稿来自James Church医生,并经过了他的同意。 [Citation ends].
[Figure caption and citation for the preceding image starts]: PJS患者小肠有蒂错构瘤可见特征性的浆膜小凹。手稿来自James Church医生,并经过了他的同意。 [Citation ends]. [Figure caption and citation for the preceding image starts]: 错构瘤息肉的组织学手稿来自Carol A.Burke医生,并经过了他的同意 [Citation ends].
[Figure caption and citation for the preceding image starts]: 错构瘤息肉的组织学手稿来自Carol A.Burke医生,并经过了他的同意 [Citation ends].
基因检测
遗传学检测用于那些符合WHO的PJS诊断标准患者的临床确诊。[14]Aaltonen LA, Jarvin H, Gruber SB, et al. Peutz-Jeghers syndrome. In: Hamilton SR, Aaltonen LA, eds. Tumors of the digestive system. Lyon, France: IACR; 2000:74-6.http://www.iarc.fr/en/publications/pdfs-online/pat-gen/bb2/bb2-chap4.pdf 对19p常染色体上编码一种丝氨酸-苏氨酸蛋白激酶的STK11(LKB1)进行基因测序,[6]Jenne DE, Reimann H, Nezu J, et al. Peutz-Jeghers syndrome is caused by mutations in a novel serine threonine kinase. Nat Genet. 1998 Jan;18(1):38-43.http://www.ncbi.nlm.nih.gov/pubmed/9425897?tool=bestpractice.com[7]Hemminki A, Makie D, Tomlinson I, et al. A serine threonine kinase gene defect in Peutz Jeghers syndrome. Nature. 1998 Jan 8;391(6663):184-7.http://www.ncbi.nlm.nih.gov/pubmed/9428765?tool=bestpractice.com 可以发现30%-69%的突变,[18]Amos CI, Keitheri-Cheteri MB, Sabripour M, et al. Genotype-phenotype correlations in Peutz-Jeghers syndrome. J Med Genet. 2004 May;41(5):327-33.http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pubmed&pubmedid=15121768http://www.ncbi.nlm.nih.gov/pubmed/15121768?tool=bestpractice.com[19]Aretz S, Stienen D, Uhlhaas S, et al. High proportion of large genomic STK11 deletions in Peutz-Jeghers syndrome. Hum Mutat. 2005 Dec;26(6):513-9.http://www.ncbi.nlm.nih.gov/pubmed/16287113?tool=bestpractice.com[20]Volikos E, Robinson J, Aittomaki K, et al. LKB1 exonic and whole gene deletions are a common cause of Peutz-Jeghers syndrome. J Med Genet. 2006 May;43(5):e18.http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=2564523&blobtype=pdfhttp://www.ncbi.nlm.nih.gov/pubmed/16648371?tool=bestpractice.com 缺失/复制分析可以发现另外30%的种系改变。[19]Aretz S, Stienen D, Uhlhaas S, et al. High proportion of large genomic STK11 deletions in Peutz-Jeghers syndrome. Hum Mutat. 2005 Dec;26(6):513-9.http://www.ncbi.nlm.nih.gov/pubmed/16287113?tool=bestpractice.com[20]Volikos E, Robinson J, Aittomaki K, et al. LKB1 exonic and whole gene deletions are a common cause of Peutz-Jeghers syndrome. J Med Genet. 2006 May;43(5):e18.http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=2564523&blobtype=pdfhttp://www.ncbi.nlm.nih.gov/pubmed/16648371?tool=bestpractice.com 阳性结果可确诊。 STK11基因的小片和大片缺失、插入、剪接位点和错位突变均有报道。[6]Jenne DE, Reimann H, Nezu J, et al. Peutz-Jeghers syndrome is caused by mutations in a novel serine threonine kinase. Nat Genet. 1998 Jan;18(1):38-43.http://www.ncbi.nlm.nih.gov/pubmed/9425897?tool=bestpractice.com[7]Hemminki A, Makie D, Tomlinson I, et al. A serine threonine kinase gene defect in Peutz Jeghers syndrome. Nature. 1998 Jan 8;391(6663):184-7.http://www.ncbi.nlm.nih.gov/pubmed/9428765?tool=bestpractice.com
阴性结果显著降低了诊断为 PJS 的可能性,但可能遗漏变异型突变。还可能发现意义不明确 (variant mutation of uncertain significance, VUS) 的变异型突变。
如果患者基因检测结果为阴性或者 VUS,并符合 WHO 标准,[14]Aaltonen LA, Jarvin H, Gruber SB, et al. Peutz-Jeghers syndrome. In: Hamilton SR, Aaltonen LA, eds. Tumors of the digestive system. Lyon, France: IACR; 2000:74-6.http://www.iarc.fr/en/publications/pdfs-online/pat-gen/bb2/bb2-chap4.pdf 那么应该按照 PJS 处理或者进一步评估是否患有其他遗传性综合征。
有研究评估了突变或者突变类型和发病风险之间的关系。 PJS没有明确的基因型-表型相关性。[4]Mehenni H, Resta N, Guanti G, et al. Molecular and clinical characteristics in 46 families affected with Peutz-Jeghers syndrome. Dig Dis Sci. 2007;52:1924-1933.http://www.ncbi.nlm.nih.gov/pubmed/17404884?tool=bestpractice.com[5]Hearle N, Schumacher V, Menko FH, et al. Frequency and spectrum of cancers in the Peutz-Jeghers syndrome. Clin Cancer Res. 2006;12:3209-3215.http://clincancerres.aacrjournals.org/cgi/content/full/12/10/3209http://www.ncbi.nlm.nih.gov/pubmed/16707622?tool=bestpractice.com 在一项纳入 51 例患者的研究中发现,与有截短突变或未发现突变的个体相比,有错义突变的个体更可能在较大的年龄出现症状,并且需要行首次息肉切除术的时间也更晚。[18]Amos CI, Keitheri-Cheteri MB, Sabripour M, et al. Genotype-phenotype correlations in Peutz-Jeghers syndrome. J Med Genet. 2004 May;41(5):327-33.http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pubmed&pubmedid=15121768http://www.ncbi.nlm.nih.gov/pubmed/15121768?tool=bestpractice.com 另一项包含419名个体(297名个体存在突变)的研究发现STK11突变的类型或位点均不能影响肿瘤的发生风险。[5]Hearle N, Schumacher V, Menko FH, et al. Frequency and spectrum of cancers in the Peutz-Jeghers syndrome. Clin Cancer Res. 2006;12:3209-3215.http://clincancerres.aacrjournals.org/cgi/content/full/12/10/3209http://www.ncbi.nlm.nih.gov/pubmed/16707622?tool=bestpractice.com STK11突变的患者和没有检测到突变的患者相比,累积肿瘤风险是相似的。
一旦在先证者身上发现突变,对于存在风险的家庭成员,可检测这种家族特异性的改变。应意识到,虽然 50% 的病例存在一名患病的父母,但是有 50% 的患者存在新发突变。对于推定是由于新突变而获病患者的父母,需要仔细评估有无 PJS 的特征(结肠息肉或皮肤黏膜色素沉着)。如果双亲中一人受累,先证者的兄弟姐妹也应接受检测。
无论是遗传还是新突变,先证者的所有子女均有50%的风险遗传突变基因,因此也需要对他们进行检测。 在进行适当的遗传咨询和知情同意后,那些存在风险的家庭成员在儿童时期就应该进行检测。Gene reviews: Peutz-Jeghers syndrome
